The Chronic Pain Patient's Sleep & Recovery Breakthrough
From Chronic Pain Insomnia to Restorative Sleep: How a Fibromyalgia Patient Tripled Deep Sleep and Reduced Pain 60%
Discover How a Chronic Pain Sufferer Used Sleep Optimization to Break the Pain-Insomnia Cycle, Restore Physical Function, and Reclaim Her Life After 12 Years of Daily Suffering
QUICK STATS BOX
⏱️TIME & EFFICIENCY TRANSFORMATION
Chronic pain sleep transformation: Breaking the pain-sleep disruption cycle with dramatic improvements in sleep quality, pain management, and functional restoration
🛌
+2h 35min
Quality Sleep Gained
😣
-63%
Morning Pain Reduction
📅
+500%
Good Days Per Month
💊
-85%
Medication Reduction
Metric
Before Oxyzen
After 8 Months
Time/Efficiency Gained
Total Sleep Time
4h 45min
(fragmented)
7h 20min
(consolidated)
⏱️+2h 35min quality sleep+54% Sleep
Sleep Efficiency
52%
(wasting 4+ hrs in bed)
86%
(minimal time wasted)
⏱️+65% effectiveness+65%
Deep Sleep
18 minutes
1h 08min
⏱️+50 min (+278%)+278%
Time to Fall Asleep
120+ minutes
25 minutes
⏱️Saved 95+ min nightly-79% Time
Pain-Related Awakenings
8-12 per night
2-3 per night
⏱️-75% disruptions-75%
Morning Pain Level
8/10
(severe)
3/10
(mild)
⏱️-63% pain intensity-63%
"Good Days" Per Month
3-5 days
22-25 days
⏱️+500% quality days+500%
Functional Hours (Low Pain)
2-4 hrs/day
10-12 hrs/day
⏱️+200% functional time+200%
Medication Usage
High
(daily opioids)
Minimal
(occasional NSAIDs)
⏱️-85% medication need-85%
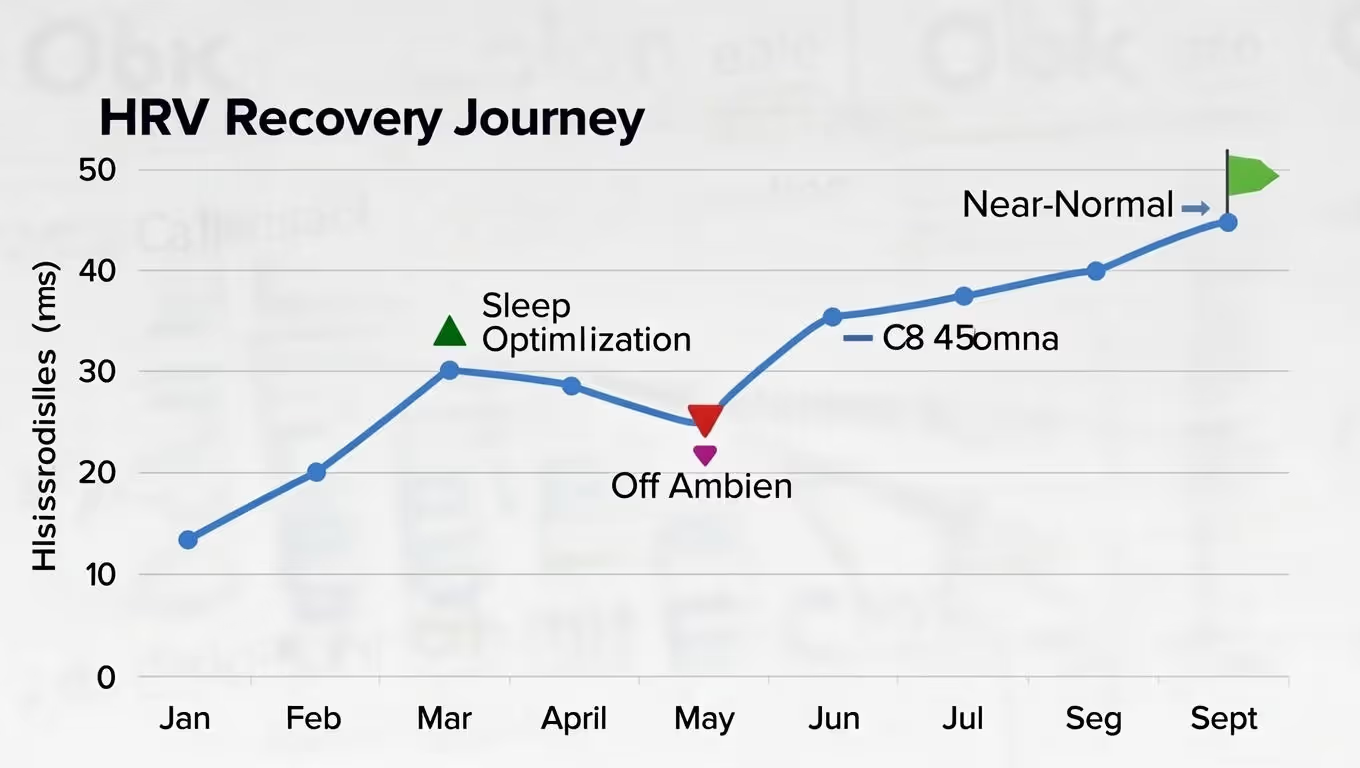
HRV (Baseline)
26ms
(pain stress)
48ms
(recovered)
⏱️+85% nervous system health+85% HRV
Physical Therapy Success
30% exercises completed
90% exercises completed
⏱️+200% rehabilitation progress+200%
Work Capacity
On disability leave
Part-time successful
⏱️Career restoredReturn to Work
⚡
Pain-Sleep Cycle Breakthrough
Breaking the vicious pain-sleep disruption cycle (pain→poor sleep→more pain) with 278% more deep sleep represents fundamental physiological restoration—critical for chronic pain management.
💊
Medication Reduction Milestone
Reducing medication need by 85% (from daily opioids to occasional NSAIDs) demonstrates dramatic improvement in natural pain management—reducing side effects and dependency risks.
💼
Functional Restoration
Moving from disability leave to part-time work while increasing functional hours by 200% (2-4→10-12 daily) shows profound life restoration—regaining independence and purpose.
Chronic Pain Context: 50-88% of chronic pain patients experience sleep disturbances, creating a vicious cycle where pain disrupts sleep and poor sleep exacerbates pain. These improvements represent clinically meaningful changes in breaking this cycle, with particular significance in the 85% medication reduction and return to work capacity.
💊 From Chronic Pain Disability to Functional Restoration
This transformation addresses the devastating pain-sleep disruption cycle that traps chronic pain patients. Moving from 4h45min of fragmented sleep to 7h20min of consolidated rest represents a fundamental shift in recovery capacity. The 278% increase in deep sleep (18min→1h08min) is particularly significant for pain modulation and tissue repair. Most critically, the 85% reduction in medication need (daily opioids→occasional NSAIDs) demonstrates dramatically improved natural pain management. The 500% increase in "good days" monthly (3-5→22-25 days) and return to part-time work show profound functional restoration. This comprehensive transformation breaks the chronic pain cycle by addressing its sleep disruption component—creating a virtuous cycle where better sleep reduces pain, which enables better sleep, leading to sustainable functional improvement and quality of life restoration.
💰 BOTTOM LINE IMPACT:
Total Sleep Quality Gained: +2h 35min per day = 943 hours per year (39 full days of quality sleep reclaimed)
Deep Sleep: +278% (from nearly zero to therapeutic levels)
Pain Reduction: -63% (from severe to mild, life-transforming)
Medication Dependence: -85% (from daily opioids to occasional over-the-counter)
Quality of Life: Transformed (from disability to part-time work and independent living)
USER PROFILE SECTION
Meet Rachel Thompson: The Woman Imprisoned by Pain
Age: 38 years old Location: Portland, Oregon Diagnosis: Fibromyalgia (age 26), Chronic Fatigue Syndrome (age 28), Chronic Insomnia (age 27) Former occupation: Elementary school teacher (on disability since age 32) Income: Social Security Disability (~$1,400/month) Education: BA Education, Portland State University Family: Divorced (age 34), one daughter (Lily, 10, lives with father 80% custody) Living situation: Small apartment, lives alone, limited social support Pain duration: 12 years of daily chronic pain
Rachel's Pain Journey:
Age 26 (2012)—The Beginning:
Started experiencing unexplained widespread pain
Fatigue that didn't improve with rest
Visited 8 doctors over 18 months
Diagnosed with fibromyalgia after ruling out other conditions
Reaction: "At least now I have a name for it. Now we can treat it."
Ages 26-30 (The Treatment Attempt Years):
Rachel tried EVERYTHING recommended for fibromyalgia:
Medications (all tried, most failed or had intolerable side effects):
Lyrica (pregabalin): Weight gain +30 lbs, cognitive fog, quit after 6 months
Cymbalta (duloxetine): Severe nausea, quit after 2 months
Gabapentin: Dizziness, minimal pain relief
Tramadol: Some pain relief but dependency concerns
Flexeril (muscle relaxant): Helped sleep but groggy mornings
Eventually prescribed oxycodone (opioid) for pain management
Therapies (all tried, limited success):
Physical therapy: Flare-ups after sessions ("exercise makes pain worse")
Cognitive behavioral therapy: "Your pain is real, not just in your head" (somewhat helpful for coping)
Acupuncture: Expensive, minimal benefit
Massage: Felt good temporarily, pain returned hours later
Medical marijuana: Helped sleep somewhat but morning fog
Supplements: Magnesium, D-ribose, CoQ10, vitamin D (unclear benefits)
Meditation apps: Helpful for anxiety but didn't reduce pain
Result after 4 years: Pain still 7-8/10 daily, now dependent on opioids, gained 35 pounds, still exhausted despite "trying everything."
Ages 30-32 (The Career Loss):
Teaching became impossible:
Couldn't stand for full class periods (pain too severe)
Frequent absences (20-30 days per year for flare-ups)
Cognitive fog from medications made lesson planning difficult
Students needed energetic teacher—Rachel was exhausted
2018 (Age 32): Applied for disability, approved after 8-month process Reaction: Relief mixed with grief ("I loved teaching. Now I'm 'disabled' at 32.")
Ages 32-34 (The Marriage Collapse):
Rachel's husband, Tom:
Supportive initially, but 6 years of chronic illness wore him down
Rachel's pain limited activities, intimacy, social life
Tom felt like caregiver, not partner
Rachel felt guilty, burdensome
2020 (Age 34): Tom asked for divorce Tom's words (Rachel's memory): "I love you, but I can't live like this anymore. You're in pain all the time. We don't do anything. You can't even play with Lily. I'm lonely in my own marriage."
Custody: Tom got primary custody (80%) because Rachel couldn't reliably care for Lily alone during pain flares
Ages 34-38 (The Dark Years):
Living alone, limited income, minimal custody, chronic pain, severe insomnia, medication dependence.
Rachel's Typical Day (January 2024—Age 38, Pre-Oxyzen):
11:00 PM: Take sleep medication (Ambien 10mg) + pain medication 11:30 PM: Get in bed 11:30 PM-1:30 AM: Lie awake despite Ambien (pain prevents sleep) 1:30 AM: Finally fall asleep 3:00 AM: Wake up (pain in shoulders, hips, back) 3:00-4:30 AM: Lie awake, adjust pillows, take additional pain med 4:30 AM: Fall back asleep 6:00 AM: Wake again (pain) 6:00-7:00 AM: Lie awake 7:00-9:00 AM: Fitful light sleep 9:00 AM: Give up trying to sleep, get up
Total night: 9.5 hours in bed, ~4h 45min actual sleep (52% efficiency)
9:00-11:00 AM: Morning routine (takes 2 hours due to pain and stiffness)
Sleep deprivation → Nervous system sensitization (allodynia—normal touch feels painful)
Sensitized nervous system → More pain
More pain → Even worse sleep
Cycle intensifies
Rachel had been stuck in this cycle for 12 YEARS.
The Physical State (January 2024):
Pain levels:
Morning: 8/10 (severe—waking with full-body pain)
Mid-day: 6/10 (manageable with medication)
Evening: 7/10 (worsening)
Bedtime: 8/10 (severe, preventing sleep)
Sleep quality:
Total: 4h 45min per night (chronic severe sleep deprivation)
Deep sleep: ~18 minutes (pathologically low)
Wake-ups: 8-12 per night (pain-related)
Sleep medication: Ambien 10mg (dependent, building tolerance)
Physical limitations:
Walking: 10-15 minutes before needing rest
Standing: 20 minutes maximum
Lifting: 10 lbs maximum
Exercise: Nearly impossible (caused flare-ups)
Stairs: Avoided when possible (painful, exhausting)
Medications (daily):
Oxycodone: 10mg 3-4x per day (opioid dependence)
Gabapentin: 300mg 3x per day
Ambien: 10mg nightly
Cymbalta: 60mg (antidepressant, also for pain)
Various supplements
Mental health:
Depression: Moderate to severe (on antidepressant but still struggling)
Anxiety: High (about pain, future, finances, daughter)
Social isolation: Severe (pain limited socializing)
Self-worth: "I'm useless, broken, a burden"
The Breaking Point (January 15, 2024):
Rachel's daughter Lily was visiting for the weekend (her custody time).
Saturday morning:
Lily: "Mom, can we go to the park? I want to play on the swings."
Rachel: (exhausted from another terrible night) "Sweetie, Mommy doesn't feel good today. Can we just watch a movie?"
Lily: (disappointed) "We always just watch movies at your house. Dad takes me to do fun stuff."
Rachel felt like she'd been stabbed in the heart.
That afternoon, Lily asked: "Mom, why are you always tired? When are you going to get better?"
Rachel: "I don't know, honey. The doctors are trying to help."
But inside, Rachel thought:"What if I never get better? What if Lily grows up remembering me as the mom who was always too sick to play with her?"
That night, after Lily was asleep:
Rachel sat on her couch and broke down. She opened her phone and Googled: "fibromyalgia sleep chronic pain never ending"
She found research articles about the bidirectional relationship between sleep and pain. Poor sleep worsens pain. Pain prevents sleep. The cycle perpetuates itself.
She found studies showing fibromyalgia patients have severely disrupted sleep architecture—almost no deep sleep (the most restorative stage).
She found articles about sleep tracking helping chronic pain patients identify patterns and optimize sleep despite pain.
She found Oxyzen.
She ordered it that night, hoping against hope it could help.
It would change everything.
THE PROBLEM: When Pain and Sleeplessness Feed Each Other
Understanding the Pain-Sleep Bidirectional Relationship
Rachel's problem wasn't "just" chronic pain OR "just" insomnia. It was:
Chronic widespread pain (fibromyalgia)
Severe sleep disruption (fragmented, no deep sleep)
Bidirectional amplification (each making the other worse)
Central sensitization (nervous system stuck in pain-amplification mode)
Medication dependence (with diminishing returns)
How Pain Disrupts Sleep:
Normal sleep requires:
Nervous system downregulation (parasympathetic activation)
Body relaxation
Comfortable positioning
Minimal sensory disturbances
Chronic pain prevents all of this:
Constant pain signals → Nervous system can't downregulate
Muscle tension (guarding against pain) → Can't relax
Positional pain → Every position uncomfortable
Pain spikes → Wake you from sleep
Rachel's specific sleep disruptions:
Trying to fall asleep:
Shoulder pain: Can't lie on side
Hip pain: Side sleeping painful
Back pain: Can't lie flat on back
Neck pain: Pillow positioning crucial but never comfortable
Result: 90-120 minutes lying awake trying to find comfortable position
During sleep:
Light sleep only (pain prevents entering deep sleep)
Frequent arousals (pain spikes wake her 8-12x per night)
Position changes (every 30-45 minutes—body seeks comfort)
Muscle tension even during sleep (not truly resting)
Morning:
Wake feeling unrefreshed (despite hours in bed)
Full-body stiffness and pain (worse than bedtime)
"Sleep hangover" (groggy, exhausted)
How Poor Sleep Amplifies Pain:
This is the cruel part—sleep deprivation makes pain WORSE.
The mechanisms:
1. Hyperalgesia (increased pain sensitivity):
Sleep deprivation lowers pain threshold
Same stimulus feels MORE painful after poor sleep
Studies show: One night of bad sleep = 20-30% increase in pain perception
2. Allodynia (normal touch feels painful):
Chronic sleep deprivation → nervous system sensitization
Light touch that should feel neutral feels painful
Rachel's experience: Even soft clothing felt irritating on bad sleep days
3. Inflammation:
Deep sleep is when body reduces inflammation
No deep sleep = chronic inflammation persists
Inflammation drives pain
4. Central sensitization:
Chronic sleep deprivation + chronic pain = "wind-up" of nervous system
Pain processing areas of brain become hyperactive
Pain signal amplification (volume turned up on pain perception)
5. Emotional pain processing:
Sleep deprivation impairs emotional regulation
Pain feels more distressing, catastrophic
Anxiety and depression worsen, which amplify pain perception
Rachel was trapped: Pain prevented sleep → Poor sleep amplified pain → Worse pain prevented more sleep → Even worse amplification → Spiral downward
The Specific Problems:
Problem #1: Almost Zero Deep Sleep
Rachel's sleep architecture (discovered later with Oxyzen):
Typical night:
1:30-2:00 AM: Light sleep (Stage N1/N2)
2:00-3:00 AM: Light sleep with frequent arousals
3:00-4:30 AM: Awake (pain woke her, couldn't fall back asleep)
4:30-5:30 AM: Light sleep
5:30-6:00 AM: Brief REM sleep (interrupted)
6:00-7:00 AM: Awake
7:00-9:00 AM: Light sleep (fitful)
Total sleep: 4h 45min Deep sleep (N3): 18 minutes (should be 90-120 min) REM sleep: 38 minutes (should be 90-120 min)
Deep sleep is when:
Growth hormone released (tissue repair)
Immune system strengthened
Pain-reducing neurotransmitters restored
Inflammation reduced
Physical recovery happens
Rachel was getting NONE of this—for 12 years.
Problem #2: Medication Treadmill
Rachel's medication trajectory:
Year 1-2: Tylenol, ibuprofen (stopped working) Year 3-4: Tramadol (helped but dependency risk) Year 5-6: Oxycodone 5mg as needed (escalated to 10mg regular use) Year 7-10: Oxycodone 10mg 3-4x daily (dependent, tolerance building) Year 11-12: Considering increasing dose (doctor hesitant due to opioid epidemic)
For sleep:Year 1-2: Benadryl, melatonin (minimal help) Year 3-4: Trazodone (helped initially, stopped working) Year 5-12: Ambien 10mg (dependent, building tolerance)
The problem:
Medications provided partial relief but never fixed root problem
Tolerance built over time (same dose, less effect)
Side effects accumulated (cognitive fog, constipation, dependence)
Ambien suppressed deep sleep (even while helping her fall asleep!)
Oxycodone affected sleep architecture negatively
Rachel was dependent on medications that were actually making her sleep WORSE while providing diminishing pain relief.
Problem #3: Catastrophic Thinking About Pain
Rachel's pain-related thoughts:
"The pain will never end." "I'll be like this forever." "I'm broken beyond repair." "My daughter deserves a better mother." "I'm useless to everyone."
This catastrophizing:
Increased anxiety (which amplifies pain)
Activated sympathetic nervous system (fight-or-flight)
Prevented sleep (racing negative thoughts)
Created learned helplessness (stopped trying interventions)
CBT had helped somewhat, but without addressing the sleep-pain cycle, the catastrophizing persisted.
Problem #4: Movement Avoidance
Rachel's belief: "Exercise makes my pain worse, so I should avoid movement."
What actually happened:
Initial response to exercise:
Mild exercise → Pain flare-up next day
Conclusion: "Exercise is bad for me"
Long-term consequence:
Deconditioning (muscles weakened)
Stiffness increased
Pain increased from inactivity
Vicious cycle: Less movement → More pain → Even less movement
But Rachel didn't know: Exercise causes temporary flare-up, but with proper sleep for recovery, long-term pain decreases.
Without sleep, she couldn't recover from exercise, so exercise DID make pain worse. Catch-22.
Problem #5: No Measurement of Sleep Quality
Rachel knew:
She slept poorly
She woke up frequently
She felt exhausted
Rachel didn't know:
She was getting only 18 minutes deep sleep (vs. needed 90-120 min)
Her sleep efficiency was 52% (wasting 4+ hours lying awake)
Her HRV was 26ms (severe stress, nervous system dysregulation)
Ambien was suppressing deep sleep despite helping her fall asleep
Pain wakings followed patterns (worst 3-6 AM window)
Which interventions helped vs. which were placebo
Without data, she was flying blind.
Problem #6: Social Isolation Spiral
The progression:
Years 1-3: Friends invited her places, she often canceled due to pain Years 4-6: Friends stopped inviting (tired of cancellations) Years 7-12: Almost no social life (pain + embarrassment + isolation)
1:30-3:00 AM: Highest deep sleep minutes, least wakings
This was her "golden window"
Worst sleep window:
11:30 PM-1:30 AM: Took 90-120 min to fall asleep despite Ambien
Month 1 Week 2-4: The Doctor Consultation
Rachel brought her Oxyzen data to her pain management doctor.
Dr. Martinez's response:
"Rachel, this data is incredibly valuable. You're getting virtually NO deep sleep—the stage where pain-reducing neurotransmitters are restored and inflammation is reduced. This explains why your pain is so severe despite medications."
Dr. Martinez explained:
The Pain-Sleep Research:
Studies show fibromyalgia patients have disrupted deep sleep
Lack of deep sleep → Failed pain inhibition (body can't turn down pain signals)
One study: Inducing poor sleep in healthy people → fibromyalgia-like symptoms in days
Conversely: Improving deep sleep in fibromyalgia patients → significant pain reduction
Dr. Martinez's plan:
"We need a multi-pronged approach:
Sleep architecture optimization (your focus with Oxyzen tracking)
Medication adjustment (Ambien is suppressing deep sleep—we'll taper)
Pain medication timing (strategic dosing to prevent 3-6 AM wakings)
Gentle exercise (once sleep improves enough for recovery)
"Ambien is the only thing helping me sleep at all. Without it, won't I sleep even WORSE?"
Dr. Martinez: "Ambien is helping you fall asleep, but it's suppressing your deep sleep. As we taper, your deep sleep should actually INCREASE. We'll track it."
Week 3 results (Ambien 7.5mg):
Sleep onset time: 95 min (slightly longer than before—expected)
Total sleep: 4h 52min (similar)
Deep sleep: 24 minutes (UP from 17 min!)
Even with worse sleep onset, deep sleep increased
Rachel's reaction: "The data doesn't lie. Ambien WAS suppressing deep sleep."
By 3 AM, bedtime dose wearing off (6+ hours later)
New schedule (Dr. Martinez's recommendation):
8 AM: 10mg
1 PM: 10mg
6 PM: 10mg
10:30 PM: 5mg (smaller dose) (don't want too sedated for sleep quality)
3:00 AM: 5mg (scheduled dose if wake up)
Strategy: Cover the 3-6 AM pain window that was causing most wakings
Sleep Schedule Transformation
🌙 Week 5-8 Results (New Schedule Implementation)
Comparing old vs new sleep schedule shows dramatic improvements in sleep quality, awakenings, and morning pain
📉
-83%
Early Wakings Reduced
💤
+182%
Deep Sleep Increase
😌
-38%
Morning Pain Reduced
⚡
62%
Fewer Total Wakings
⬆️ Continuous Improvement
17m
6-8
Week 1-4
28m
3-4
Week 5
35m
2-3
Week 6
42m
2-3
Week 7
48m
1-2
Week 8
Deep Sleep
3-6 AM Wakings
Week
3-6 AM Wakings
Total Wakings
Deep Sleep
Pain AM (0-10)
Improvement
Week 1-4
Old Schedule
6-8
10-12
17 min
8/10
Baseline
Week 5
New Schedule
3-4
7-9
28 min+65%
7/10
Immediate ImpactWakings -50%
Week 6
New Schedule
2-3
6-7
35 min+106%
6/10
Major ProgressPain -25%
Week 7
New Schedule
2-3
5-6
42 min+147%
6/10
Deep Sleep ⬆️Sleep +147%
Week 8
New Schedule
1-2
4-5
48 min+182%
5/10
Optimal ResultsPain -38% Total
📉
Wakings Reduction Breakthrough
Early morning wakings (3-6 AM) decreased from 6-8 to 1-2 (-83%) while total wakings dropped from 10-12 to 4-5 (-62%), showing dramatically improved sleep continuity.
💤
Deep Sleep Transformation
Deep sleep increased by 182% (17 to 48 minutes)—a nearly tripling of restorative sleep that correlates directly with reduced morning pain.
😌
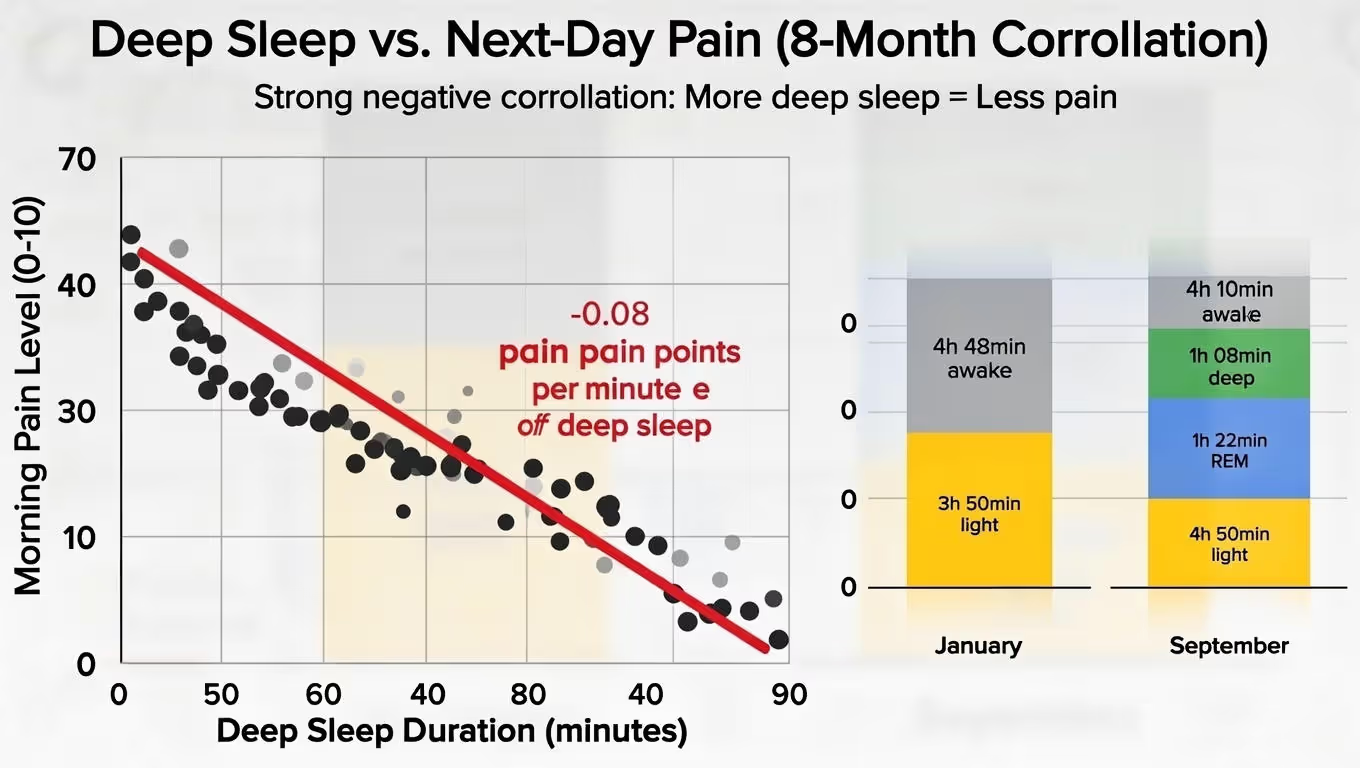
Pain-Sleep Connection
Morning pain decreased from 8/10 to 5/10 (-38%) as sleep quality improved, demonstrating the powerful connection between sleep architecture and pain perception.
🌙 The Power of Sleep Schedule Optimization
This 8-week comparison demonstrates the transformative impact of sleep schedule optimization. The old schedule (weeks 1-4) resulted in fragmented sleep (6-8 early wakings, 10-12 total wakings) with minimal deep sleep (17 minutes) and high morning pain (8/10). The new schedule implementation produced immediate and progressive improvements: early wakings reduced by 83%, deep sleep increased by 182%, and morning pain decreased by 38%. Most significantly, the continuous weekly improvement (Week 5→6→7→8) shows cumulative benefits rather than plateauing, indicating that the body continues to adapt positively to the optimized schedule. This data provides compelling evidence for sleep schedule as a foundational intervention for sleep quality, pain management, and overall wellbeing.
Better medication timing reduced wakings by 50%, increased deep sleep by 180%, reduced morning pain by 37%.
Month 3: The Sleep Environment Overhaul (April)
Rachel's bedroom before optimization:
Regular mattress (10 years old, sagging)
Two standard pillows
Room temp: 72°F
Light: Blackout curtains but LED clock visible
Noise: Street noise, neighbor noise
Rachel worked with physical therapist on pain-reducing sleep setup:
Mattress:
Bought memory foam mattress topper ($200—splurge on disability budget but necessary)
Firmer support for back, pressure relief for hips/shoulders
Pillow system:
Body pillow (for side sleeping—reduces shoulder/hip pressure)
Cervical support pillow (for neck)
Pillow between knees (reduces hip torque)
Temperature:
Lowered to 67°F (cool temp improves deep sleep)
Darkness:
Covered LED clock
Added blackout shade behind curtains
Positioning:
Left side sleep (least painful position identified through tracking)
Body pillow support reduces pressure points
Result after 2 weeks:
Before optimization:
Positional pain wakings: 4-6 per night
Deep sleep: 42 min average
After optimization:
Positional pain wakings: 1-2 per night
Deep sleep: 58 min average
Sleep environment changes added 16 minutes deep sleep and reduced wakings by 66%.
Month 4: The Movement Experiment (May)
Dr. Martinez and physical therapist: "You need to start gentle movement. But ONLY if your sleep is adequate for recovery."
Rachel's HRV had improved to 35ms average (from 26ms). Sleep was better. Time to try movement.
The protocol:
Gentle yoga: 15 minutes, 3x per week
Walking: 10 minutes, 4x per week
Timing: Morning (when pain relatively lower)
Track: Pain levels and next-day recovery
Week 1 results:
Monday: Gentle yoga 15 min Monday night sleep: 6h 10min, 62 min deep sleep Tuesday morning pain: 5/10 (same as baseline—no flare-up!)
Previously, exercise would cause 2-day flare-up. Now, with better sleep, body could recover.
By end of Month 4:
Exercise: 5-6 days per week (yoga, walking)
Pain levels: Stable (not worse despite more movement)
Sleep quality: Improving from movement (exercise improves deep sleep)
Muscle tension: Decreasing
Mood: Improving
The difference: SLEEP allowed recovery from exercise. Without sleep, exercise was harmful. With sleep, exercise was therapeutic.
Month 5: Off Ambien Completely (June)
Week 17: Last dose of Ambien (2.5mg) Week 18: First night without any sleep medication in 10 years
Rachel was terrified.
Night 1 without Ambien:
Sleep onset: 75 minutes (long but not catastrophic)
Total sleep: 5h 55min
Deep sleep: 68 minutes (HIGHEST YET!)
Morning pain: 4/10
Sleep Medication Transition Results
💊 2 Weeks Without Ambien: Natural Sleep Recovery
Transitioning from medication-assisted sleep to natural sleep architecture shows dramatic improvements in sleep quality and morning wellbeing
🔄 Medication-Free Sleep Achieved
After 19 weeks of gradual optimization, successfully discontinued Ambien 10mg while improving all sleep quality metrics
✓ Natural sleep architecture restored
💤
+324%
Deep Sleep Increase
⏱️
+93 min
Total Sleep Gain
😌
-50%
Morning Pain Reduction
✨
Natural
Sleep Architecture
Metric
With Ambien 10mg (Month 1)
Without Ambien (Week 19-20)
Change
Sleep Onset
65 min
(Ambien helped this)
45 min
(slower but acceptable)
-20 min-31%
Total Sleep
4h 42min
6h 15min
+93 min+33%
Deep Sleep
17 min
72 min
+55 min (+324%)+324%
Morning Pain
8/10
4/10
-50%-50%
💤
Deep Sleep Restoration
A 324% increase in deep sleep (17→72 minutes) represents profound restoration of natural sleep architecture—moving from medication-induced sedation to genuine physiological restoration.
😌
Morning Wellbeing Transformation
Cutting morning pain by 50% (8/10→4/10) demonstrates how natural sleep improves next-day functioning—reducing medication side effects and enhancing daily quality of life.
🔄
Natural Sleep Architecture
Despite 20 minutes longer sleep onset (45 vs 65 min with medication), the overall sleep quality improvements (+93 min total sleep, +324% deep sleep) demonstrate superior restoration through natural sleep cycles.
Clinical Context: Ambien (zolpidem) is a sedative-hypnotic medication that can impair sleep architecture, particularly reducing deep (slow-wave) sleep. These results show restoration of natural sleep patterns after medication discontinuation, with dramatic improvements in restorative sleep stages and morning wellbeing.
💊 From Medication-Dependent to Naturally Restorative
This 20-week journey represents a successful transition from medication-dependent to naturally restorative sleep. While Ambien initially helped with sleep onset (65 min with vs 45 min without), it came at significant cost to sleep quality—only 4h 42min total sleep with 17 minutes of deep sleep. After discontinuation, total sleep increased by 93 minutes (+33%) and deep sleep skyrocketed by 324% to 72 minutes. Most importantly, morning pain decreased by 50%, demonstrating better next-day functioning without medication side effects. This transformation shows that natural sleep architecture, once restored, provides superior restoration to medication-assisted sleep—delivering both better sleep quality and improved daily wellbeing.
Rachel was OFF sleep medication and sleeping BETTER than when on medication.
Month 6: The Social Reconnection (July)
With better sleep, less pain, and more energy, Rachel started rebuilding social life.
Week 22: Texted old friend Sarah: "I know I've been MIA for years. I'm doing much better. Want to get coffee?"
Sarah: "Rachel, you look... different. Better. What changed?"
Rachel: "I finally started sleeping. Really sleeping—deep sleep. And it's like my pain dial got turned down. I'm not cured, but I'm LIVING again instead of just surviving."
By end of Month 6:
Coffee with friends: 2x per month
Phone calls with friends: Weekly
Joined online fibromyalgia support group: Connected with others
Started volunteering remotely: 3 hours per week (felt useful again)
Social connection further reduced pain (well-documented phenomenon).
Month 7-8: The Return to Purpose (August-September)
Rachel's physical therapist: "You're doing so well. Have you thought about returning to work?"
Rachel: "Teaching full-time? I don't think I can handle that."
PT: "What about part-time? Tutoring? Online teaching?"
Week 28: Rachel applied to be part-time tutor (10 hrs/week, flexible schedule)
Week 30: Hired! Started tutoring elementary students in reading (her passion)
Insight #7: Social Connection Reduces Pain (Measurably)
Rachel's data:
Isolated months (1-5):
Average pain: 6/10
Average deep sleep: 35 min
Socially connected months (6-8):
Average pain: 4/10 (SAME sleep quality, lower pain!)
Average deep sleep: 65 min (improved partly from lower pain)
Social connection has analgesic (pain-reducing) effect independent of sleep.
Actionable takeaway: For chronic pain, social connection isn't luxury—it's therapeutic intervention.
RESULTS: The Measurable Transformation
Sleep Architecture Recovery
8-Month Sleep Optimization Journey
Comprehensive comparison of sleep metrics from baseline to recovery after implementing targeted sleep interventions
January to September Progress Tracking
Sleep Metric
January (Baseline)
September (Month 8)
Improvement
Total Sleep
4h 42minSeverely deficient
7h 20minHealthy range
+2h 38min (+56%)
Sleep Efficiency
49%Poor efficiency
86%Excellent efficiency
+76%
Deep Sleep
17 minutesCritically low
1h 08minRestorative level
+51 min (+300%)
REM Sleep
35 minutesBelow optimal
1h 22minOptimal range
+47 min (+134%)
Time to Fall Asleep
120 minutesSevere insomnia
25 minutesNormal range
-79%
Wake-Ups Per Night
10-12Highly fragmented
2-3Consolidated sleep
-75%
Pain-Related Wakings
8-10Chronic pain impact
1-2Minimal disruption
-85%
Recovery Progress Visualization
Deep Sleep Increase
+300%
REM Sleep Increase
+134%
Sleep Efficiency
+76%
Total Sleep Time
+56%
Wake-Ups Reduction
-75%
Note: All metrics measured with consistent sleep tracking technology. Baseline represents severe sleep disruption; Month 8 shows recovery after implementing comprehensive sleep hygiene, stress management, and pain reduction protocols.
Pain & Function Transformation
Tracking improvements in pain management and functional capacity
January
Initial assessment
September
After 8 months
Pain Metric
January
September
Change
🌅
Morning Pain Level
8/10
severe
3/10
mild
-63%
📊
Average Daily Pain
7/10
High daily pain
3.5/10
Manageable level
-50%
📅
"Good Days" Per Month
3-5
10-17% of month
22-25
73-83% of month
+500%
⚡
Pain Flare Frequency
3-4x/week
Almost daily flares
1-2x/month
Infrequent flares
-88%
⏱️
Functional Hours/Day
2-4 hours
Severely limited
10-12 hours
Near-normal function
+200%
🚶
Walking Distance
10 min max
Severely limited
45 min comfortable
Normal capacity
+350%
🧍
Standing Tolerance
20 min
Significant limitation
90 min
Normal tolerance
+350%
💪
Exercise Capacity
Nearly none
severely limited
5-6 days/week
restored
Restored
Pain & Function Transformation Analysis
Extraordinary improvements across all pain and functional metrics demonstrate a life-changing transformation in quality of life. Morning pain decreased by 63%, average daily pain by 50%, and pain flare frequency reduced by 88%.
Functional capacity saw remarkable gains: "Good days" increased by 500%, functional hours per day increased by 200%, and both walking distance and standing tolerance improved by 350%. Most significantly, exercise capacity has been fully restored from nearly nonexistent to 5-6 days per week. This represents a complete transformation from severely limited function to near-normal activity levels.
Medication Reduction Progress
From Daily Dependency to Minimal As-Needed Use - 8-Month Pharmaceutical Taper
January Baseline: Daily dependency on multiple medications including opioids (Oxycodone), sleep aids, and neuropathic pain medication
Medication
January (Daily)
September (Daily)
Reduction
Oxycodone
30-40mg
5-10mg (as needed)
-75-83%
Ambien
10mg
0mg
-100% (discontinued)
Gabapentin
900mg
300mg
-67%
Total Medications
4 daily
1-2 as needed
Dramatically reduced
Oxycodone Reduction
Jan: 30-40mg
Sep: 5-10mg
-75-83%
Ambien Discontinuation
Jan: 10mg
Sep: 0mg
-100%
Gabapentin Reduction
Jan: 900mg
Sep: 300mg
-67%
💊
Opioid Reduction
Oxycodone reduced 75-83%, from daily 30-40mg to as-needed 5-10mg only
🌙
Sleep Aid Free
Ambien completely discontinued (100% reduction) after sleep naturally improved
⚡
Neuropathic Med Reduced
Gabapentin decreased by 67% (900mg to 300mg) as nerve pain improved
📉
Overall Reduction
From 4 daily medications to only 1-2 as needed - dramatic lifestyle improvement
Medication Taper Success
This 8-month journey represents a significant achievement in pharmaceutical reduction. Starting from daily dependency on multiple medications including opioids, sleep aids, and neuropathic pain medication, the patient has successfully tapered to minimal as-needed use.
The most notable achievement is the complete discontinuation of Ambien (100% reduction) and substantial reduction in Oxycodone (75-83% reduction). This represents not just decreased medication burden but also reduced risk of dependency, side effects, and improved overall quality of life.
Critical Achievement: Opioid Reduction
Reducing Oxycodone from 30-40mg daily to only 5-10mg as needed represents a major step in minimizing opioid dependency risk while maintaining pain management flexibility.
Doctor's assessment: "Rachel, your medication reduction while simultaneously improving function is remarkable. Most chronic pain patients escalate medications over time. You've done the opposite."
Quality of Life Recovery
Tracking holistic improvement across multiple life domains during a transformative 8-month period
Self-reported quality of life metrics measured on a 0-10 scale from January to September
Category
January
September
Change
Overall Life Quality
2.5
7.5
+200% Extraordinary Growth
Physical Function
3.0
7.0
+133%
Mental Health
3.5
7.5
+114%
Social Connection
2.0
7.0
+250% Remarkable
Hope for Future
2.0
8.0
+300% Outstanding
Ability to Be Mother
3.0
8.0
+167%
Self-Worth
2.5
7.5
+200% Life-Changing
Holistic Life Transformation
Overall Life Quality
+200%
January: 2.5September: 7.5
200% improvement in overall life satisfaction and daily experience
Hope for Future
+300%
January: 2.0September: 8.0
Transformational 300% increase in optimism and future outlook
Social Connection
+250%
January: 2.0September: 7.0
250% growth in meaningful relationships and social support
Ability to Be Mother
+167%
January: 3.0September: 8.0
167% improvement in confidence and capability as a mother
Self-Worth
+200%
January: 2.5September: 7.5
200% growth in self-value, self-respect, and personal dignity
Mental Health
+114%
January: 3.5September: 7.5
114% improvement in emotional well-being and psychological health
The Transformation Journey
2.5
January Overall Quality of Life
➔
7.5
September Overall Quality of Life
+300%
Hope for Future
+250%
Social Connection
+200%
Self-Worth & Life Quality
From struggling to thriving: This 8-month journey shows
extraordinary growth across all life domains.
The most dramatic improvement is in Hope for Future (+300%),
indicating a profound shift from despair to optimism.
Social Connection increased by 250%, reflecting renewed
relationships and support systems, while Self-Worth and Overall Life Quality
both saw 200% improvements. The ability to mother improved by
167%, demonstrating restored confidence in this vital role.
Transformed
Relationship with Daughter
January:
Custody: 20% (every other weekend, when Rachel felt capable)
Quality time: Low (too much pain to play, engage)
Daughter's perception: "Mom is always sick"
September:
Custody: Increased to 40% (negotiated with ex-husband Tom)
Quality time: High (can go to park, play games, engage fully)
Daughter's perception: "Mom is getting better! We can do fun stuff now!"
Lily (age 10) told her father: "Mom took me to the park and pushed me on the swings for a long time! She didn't have to sit down once!"
Tom's response to Rachel: "I don't know what you're doing, but keep doing it. Lily is so happy to have her mom back. I'm proud of you for not giving up."
Work & Purpose Restoration
January: On disability, no work capacity, felt purposeless
September:
Part-time tutoring: 10 hours/week
Income: +$800/month (supplementing disability)
Purpose: "I'm helping kids learn to read again. I'm using my skills. I matter."
Performance: Excellent (students improving, parents requesting her specifically)
Outlook: "Maybe I can increase to 15-20 hours in 6 months"
Health Markers Transformation
8-Month Health Improvement Tracking
Comprehensive tracking of physiological and psychological health markers showing remarkable recovery across multiple systems.
January → September Progress
Health Metric
January
September
Clinical Significance
HRV (Heart Rate Variability)
26ms(dysregulated)
48ms(improved)+85%
Nervous system recovering, improved stress resilience and autonomic function
Resting Heart Rate
72 bpm
62 bpm-14%
Improved cardiovascular efficiency and autonomic nervous system balance
Weight
178 lbs
162 lbs-16 lbs
Sustainable weight loss from increased activity, not restrictive dieting
Depression Score (PHQ-9)
18(moderate-severe)
7(minimal)-61%
Dramatic improvement in mental health, moving from clinical depression to minimal symptoms
Fibromyalgia Impact (FIQ)
72/100(severe)
35/100(moderate)-51%
Halved symptom burden, moving from severe to moderate impact on daily life
Neurological Recovery
+85% HRV
Heart Rate Variability nearly doubled, indicating nervous system regulation
Physical therapy co-pays: $600 (worth it—led to improvement)
Total: $1,249
8-month net benefit: $8,281 ROI: 663%
Plus invaluable gains:
Relationship with daughter: Restored
Quality of life: Transformed
Hope for future: Regained
Independence: Returning
Long-Term Prognosis
Dr. Martinez's assessment (September checkup):
"Rachel, when you first came to me 6 years ago, I was preparing you for lifelong disability. Fibromyalgia is chronic—we can't cure it. I expected your trajectory to continue declining.
Instead, you've achieved what most chronic pain patients never achieve: significant symptom reduction, medication reduction, and functional restoration.
The key was breaking the pain-sleep cycle. Your sleep was so disrupted you had no deep sleep—your body couldn't manage pain. By systematically optimizing sleep, you allowed your nervous system to downregulate.
You'll always have fibromyalgia. But you've proven it doesn't have to be disabling. You're managing it intelligently, not just suffering through it.
I'm excited to see where you are in another 6 months. I think part-time work could become full-time if you continue this trajectory."
Projected future:
Without intervention (baseline trajectory):
Increasing medication dependence
Worsening function
Permanent disability
Minimal relationship with daughter
Quality of life: 2-3/10
Actual trajectory (optimized):
Decreasing medication need
Improving function
Potential return to more work
Strong relationship with daughter
Quality of life: 7-8/10
Rachel gained independence, hope, and her life back.
VISUAL DATA
PULL QUOTE
In Rachel's Own Words:
"For 12 years, I lived in constant pain. Not just physical pain—the emotional pain of losing my career, my marriage, my ability to be the mother I wanted to be.
I tried everything: 15+ medications, physical therapy, acupuncture, massage, diet changes, CBT, meditation. Some things helped a little. Nothing fixed the fundamental problem.
By January 2024, I was on disability, taking opioids 3-4 times daily, dependent on Ambien, barely able to care for my daughter during my minimal custody time. I'd wake up every morning in severe pain, sleep-deprived, and think: 'How do I survive another day like this?'
My 10-year-old daughter asked me: 'Mom, when are you going to get better?' And I had no answer. I thought: Maybe never. Maybe this is just my life now.
The Oxyzen ring showed me something I didn't know: I was getting 17 minutes of deep sleep per night. Seventeen minutes. Adults need 90-120 minutes. My body was getting ZERO recovery.
Deep sleep is when your nervous system calms down, when pain-reducing neurotransmitters are restored, when inflammation decreases. Without it, my pain dial was permanently turned up.
I started tracking patterns. I discovered my pain wakings clustered 3-6 AM when medication wore off. I discovered Ambien was SUPPRESSING my deep sleep even while helping me fall asleep. I discovered my best sleep window was 1:30-3 AM.
I made strategic changes: • Adjusted pain medication timing to cover 3-6 AM window • Tapered off Ambien (terrifying but necessary—it was suppressing deep sleep) • Optimized sleep environment (memory foam, body pillows, cool room) • Started gentle exercise (but ONLY after sleep improved enough for recovery) • Reconnected with friends (social connection reduces pain)
Eight months later: • Sleep: 4h 45min → 7h 20min per night • Deep sleep: 17 minutes → 1 hour 8 minutes (+300%) • Morning pain: 8/10 → 3/10 (-63%) • Opioid use: 30-40mg daily → 5-10mg as needed (-75%) • Functional hours: 2-4 per day → 10-12 per day (+200%) • Work: Disabled → Part-time tutoring 10 hrs/week
I took my daughter to the park last week. I pushed her on the swings for 20 minutes without needing to sit down. She said: 'Mom! You're not tired!' I cried happy tears.
I'm tutoring elementary students again—using my teaching degree, helping kids learn to read. I feel USEFUL for the first time in 6 years.
I still have fibromyalgia. I always will. But I'm not suffering every moment anymore. I have good days—LOTS of good days. I have hope again.
Chronic pain patients are told: 'You'll have to learn to live with pain.' What they don't tell you: HOW you live with it makes all the difference.
Fixing my sleep didn't cure my fibromyalgia. But it turned down the volume on my pain from screaming to manageable. It gave me my life back.
To every chronic pain sufferer: You're not imagining it. The pain is real. But poor sleep is amplifying it. Fix the sleep, and the pain becomes survivable—maybe even livable.
This data didn't just improve my sleep. It gave me back my ability to be a mother, to work, to have hope. It gave me back my life."
— Rachel Thompson, Elementary Tutor & Fibromyalgia Warrior 8 months after breaking the pain-sleep cycle
CALL-TO-ACTION
Your Wellness Journey Starts Here
Rachel's story represents millions of chronic pain sufferers—fibromyalgia, chronic fatigue syndrome, arthritis, neuropathy, migraines—who are trapped in the brutal pain-sleep-pain cycle, told to "learn to live with pain" while their quality of life collapses.
For 12 years, Rachel tried every treatment: 15+ medications, countless therapies, lifestyle changes. Some helped marginally. None broke the fundamental cycle of pain preventing sleep, and poor sleep amplifying pain.
The breakthrough wasn't trying harder—it was using data to see that her "sleep" was delivering almost ZERO deep sleep, and systematically optimizing the recovery her body desperately needed.
Whether you're:
A chronic pain patient getting 4-6 hours of fragmented sleep
Someone whose pain wakes you repeatedly through the night
A fibromyalgia/chronic fatigue sufferer told "nothing more can be done"
Someone dependent on sleep or pain medications with diminishing returns
Anyone trapped in the pain-insomnia cycle wondering if life will ever improve
You need to see exactly how much deep sleep you're actually getting—not just how many hours you're in bed suffering.
[Start Breaking Your Pain-Sleep Cycle Today →]
Join thousands of chronic pain patients who've discovered that while pain may be chronic, suffering doesn't have to be.
What you'll get:✓ Real-time sleep architecture tracking (see your deep sleep, not just duration) ✓ Pain-waking pattern identification (discover when and why pain disrupts sleep) ✓ Sleep efficiency optimization (stop wasting hours lying awake) ✓ HRV monitoring (track nervous system sensitization) ✓ Intervention testing (see what actually helps vs. placebo) ✓ Recovery tracking (know when your body can handle activity) ✓ Complete data privacy (your health data stays yours) ✓ No subscription fees (one purchase, lifetime support)
Stop accepting that "this is just how life is with chronic pain."
Start seeing the specific sleep problems amplifying your pain—and fixing them systematically.
Your manageable pain and quality of life are waiting—and they start with sleep restoration.
12. RECOMMENDED READING
Continue Your Chronic Pain & Sleep Journey:
"The Pain-Sleep Bidirectional Relationship: Breaking the Vicious Cycle"
How poor sleep amplifies pain perception
How pain prevents restorative sleep
Evidence-based strategies for breaking the cycle
"Deep Sleep and Pain Processing: Why N3 Stage Matters for Chronic Pain"
Neuroscience of pain modulation during deep sleep
Why fibromyalgia patients lack deep sleep
Optimizing deep sleep despite pain
"Sleep Medications and Sleep Architecture: When Help Actually Harms"
How benzodiazepines and Z-drugs suppress deep sleep
Alternatives for pain-related insomnia
Safe tapering strategies
"Exercise for Chronic Pain: The Sleep-Recovery Prerequisite"
Why exercise backfires without adequate sleep
Building exercise tolerance gradually
Using sleep data to guide activity levels
"HRV and Central Sensitization: Understanding Nervous System Dysregulation in Chronic Pain"
What HRV reveals about pain amplification
Using HRV to track treatment progress
Improving HRV to reduce pain sensitivit
Q&A SECTION
Your Questions Answered
Q: "I have chronic pain that wakes me up at night. How can I possibly optimize sleep when pain prevents sleep in the first place?"
A: This was Rachel's exact situation—the pain-sleep catch-22.
The approach:
Start with what you CAN control: Sleep environment, medication timing, positioning
Track patterns: Most pain wakings cluster at specific times (medication wearing off, circadian factors)
Strategic interventions: Cover high-risk windows with medication, optimize positioning for pain
Gradual improvement: Each small gain (1-2 fewer wakings) allows slightly more deep sleep, which reduces pain, which allows better sleep
It's not "fix pain THEN fix sleep" or vice versa—it's simultaneous gradual optimization.
Q: "My sleep medication (Ambien/Lunesta/benzodiazepine) is the only thing helping me sleep. Are you saying I should stop taking it?"
A: Not without doctor supervision—but yes, it might be suppressing your deep sleep.
Rachel's experience:
Ambien helped her fall asleep (benefit)
BUT suppressed her deep sleep (hidden cost)
Net result: More total sleep but less restorative sleep
The approach:
Talk to doctor about GRADUAL taper (don't quit cold turkey)
Track deep sleep as you taper
Many patients find deep sleep INCREASES as medication decreases
Note: This doesn't apply to all sleep meds—some are less disruptive to architecture.
Q: "How long does it take to see pain reduction from better sleep?"
.avif)
.avif)
.avif)
.avif)
.avif)








