One in Nine Australian Women Has Endometriosis. The Average Diagnosis Takes 7 Years. This Changes Now.
Endometriosis affects many Australian women, yet diagnosis takes years. Early detection through better data awareness could significantly reduce suffering and improve long-term health outcomes.
One in Nine Australian Women Has Endometriosis. The Average Diagnosis Takes 7 Years. This Changes Now.
Your cycle is trying to tell your doctor something. For 7 years, nobody listened. Now there’s data.
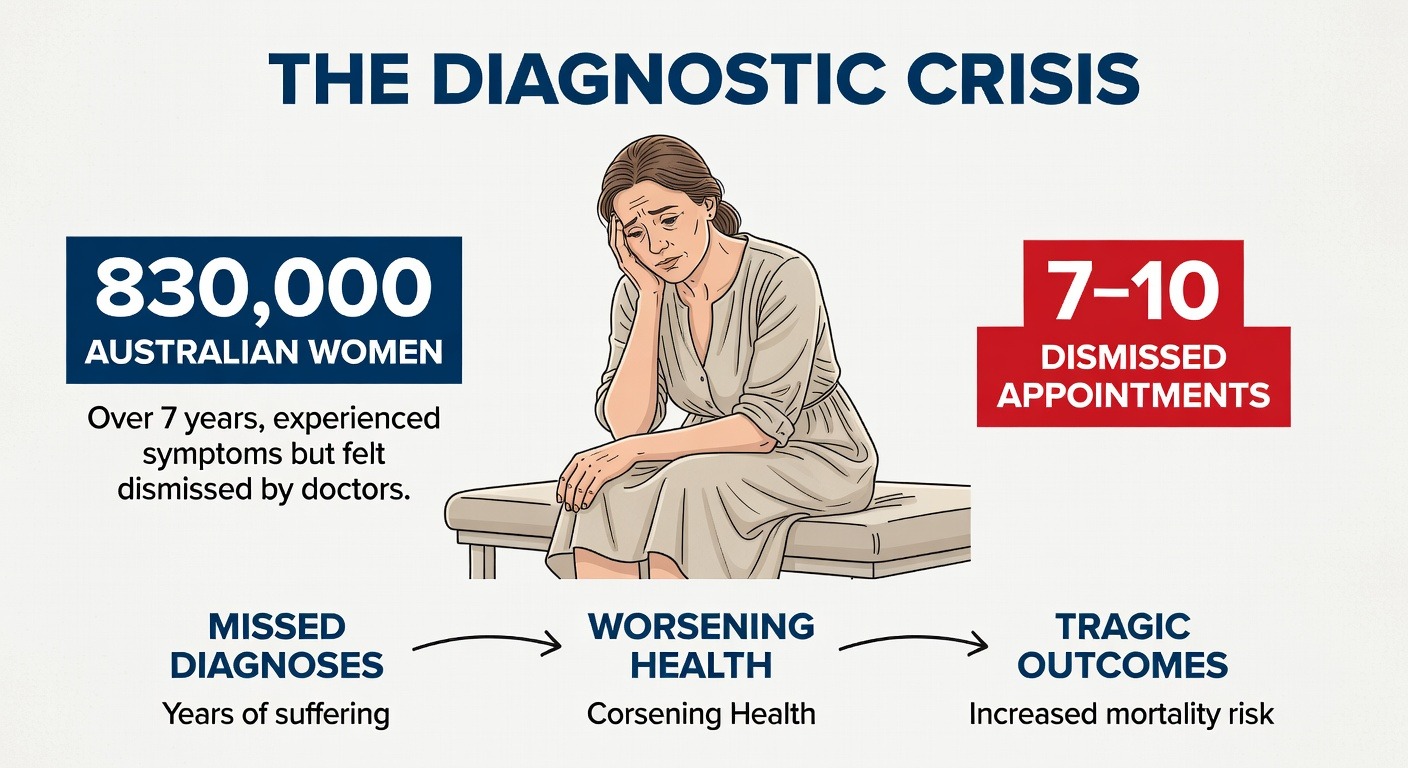
The number stops you cold when you first see it: 830,000.
That is how many Australian women are living with endometriosis right now. One in nine. More than the population of Canberra. More women than there are teachers, nurses, and police officers combined in this country. And for the vast majority of them, the journey to getting that diagnosis—simply having a name for the pain they have endured since their first period—took over seven years.
Seven years of being told it is normal. Seven years of ibuprofen and heat packs and cancelled plans. Seven years of watching friends glide through life while you cancel dinner, leave work early, or lie on the bathroom floor wondering why your body feels like it is tearing itself apart from the inside.
Here is what makes Australian women furious when they learn this statistic: endometriosis is not rare. It is not difficult to suspect. It has a known set of clinical features, a predictable pattern of symptom progression, and—contrary to what too many women have been told—it is absolutely not something you should just learn to live with.
And yet, the average Australian woman with endometriosis will see seven to ten different doctors before someone takes her seriously enough to refer her to a specialist. She will be told she has a low pain threshold. She will be offered the pill to "regulate" a cycle that is already regular but excruciating. She will be sent away with a prescription for antidepressants more often than she will be sent for an ultrasound.
This is not a failure of individual doctors. It is a failure of a system that has trained physicians to treat menstrual pain as an expected inconvenience rather than a diagnostic clue. It is a failure of a medical culture that has historically undervalued women's subjective experience of their own bodies. And it is a failure of the tools available to general practitioners—until now.
Because something has changed. For the first time, there is a way to see what your body has been trying to communicate through every cycle, every flare-up, every night of broken sleep. Your heart rate, your heart rate variability, your overnight recovery, your temperature rhythm—these biometric signals do not lie. They do not dismiss you. They do not tell you to come back when the pain is worse.
They just record. Night after night. Month after month. And when you finally bring that record to a doctor who is willing to look, the conversation changes completely.
This article is for the 830,000 Australian women waiting for answers. It is for the parents watching their teenage daughters miss school every month, wondering if this is really "just period pain." It is for the partners who have run out of ways to help. And it is for the healthcare advocates who know that seven years is seven years too long.
We are going to show you exactly what your menstrual cycle does to your heart rate and HRV every single night. We are going to walk you through the biometric signature that researchers have now identified in women with endometriosis. We are going to give you a step-by-step guide to building a GP-ready health record before your next appointment. And we are going to introduce you to four Australian women whose diagnostic journeys ended because their data finally gave them a voice in the room.
The system has not changed yet. But your ability to navigate it just did.
The Diagnostic Crisis: 830,000 Australian Women, 7 Years, 7–10 Dismissed Appointments
Let us be precise about what seven years actually means.
Seven years is approximately 2,555 days. For a woman whose symptoms began at age sixteen—and endometriosis often starts with the very first period—a seven-year diagnostic delay means she will be twenty-three before she even hears the word. That is seven years of education disrupted. Seven years of entry-level jobs where she cannot afford to take sick leave. Seven years of relationships strained by cancellations and fatigue and the quiet shame of being the friend who never shows up.
Seven years is also approximately eighty-four menstrual cycles. Eighty-four times her body sent signals that something was wrong. Eighty-four opportunities for a healthcare system to notice.
Here is what actually happens in those seven years, according to the Australian Longitudinal Study on Women's Health and the Endometriosis Australia patient registry.
The average woman with endometriosis will have her symptoms dismissed as "normal period pain" by her first GP. She will then try a second GP, hoping for a different answer. That second GP will likely prescribe an oral contraceptive, which may mask some symptoms but does not treat the underlying disease. When she returns—because the pain is still there, because the fatigue is still there, because she knows something is wrong—she will be told to "give it more time."
By doctor number four or five, she will likely be referred for a pelvic ultrasound. This ultrasound will almost certainly come back normal, because endometriosis lesions are often too small or too superficially implanted to appear on imaging. She will be told this means nothing is wrong. She will leave the appointment feeling humiliated and confused.
By doctor number six or seven, she may be told she has irritable bowel syndrome. She may be given a low-FODMAP diet to follow. She may be sent to a gastroenterologist. She may spend months eliminating foods while the real problem—endometrial-like tissue growing outside her uterus—continues to cause inflammation, adhesions, and chronic pain.
By doctor number eight or nine, she may be told the pain is psychological. She may be offered antidepressants or referred to a pain clinic that treats conditions like fibromyalgia. She may begin to doubt her own perception of her body.
And then, finally—often after she has brought a printed spreadsheet of her symptoms to an appointment, or after a partner has attended with her to advocate, or after she has found a GP who specialises in women's health—someone will say the word endometriosis. Someone will refer her to a gynaecologist. Someone will schedule a laparoscopy.
The average time from that first GP visit to the laparoscopy that confirms endometriosis? Seven point four years.
Here is the part that should make you angry: endometriosis is not difficult to diagnose in a patient who has been properly listened to. The combination of cyclic pelvic pain, painful periods, pain with intercourse, gastrointestinal symptoms that flare with menstruation, and a family history of endometriosis—this cluster of features has extremely high predictive value. A 2020 study in the Australian and New Zealand Journal of Obstetrics and Gynaecology found that when GPs used a simple symptom-screening tool, the time to diagnosis dropped by more than half.
But most GPs do not use that tool. Most GPs receive minimal training in endometriosis during medical school. Most GPs are working under time pressure, seeing twenty to thirty patients a day, and a young woman with period pain does not trigger the same urgency as chest pain or shortness of breath.
This is not malice. This is a system failure. And like most system failures, it will not be fixed by blaming individual doctors. It will be fixed by changing the information that reaches them.
That is where your data comes in.
Because here is what the system cannot ignore: a three-month record of your nightly heart rate variability, time-stamped to your menstrual cycle. A graph showing your resting heart rate climbing in the ten days before your period and crashing on day one of bleeding. A pattern of poor sleep recovery that aligns perfectly with your luteal phase. A temperature rhythm that shows the ovulatory shift is present but that your overnight parasympathetic activity is consistently suppressed compared to population norms.
This is not subjective. This is not "I feel like my pain is a seven out of ten." This is physiology. And when you walk into an appointment with a GP and place a biometric record on the desk, you change the power dynamic entirely.
You are no longer asking a doctor to believe you. You are asking a doctor to interpret data. That is what they were trained to do.
Let us look at exactly what that data shows—and why your menstrual cycle has been visible in your heart rate and HRV this entire time, even when no one was looking.
What Your Menstrual Cycle Is Actually Doing to Your Heart Rate and HRV Every Night
You have probably never thought about your heart rate variability in relation to your period. Most women have not. Most doctors have not. But the relationship between the menstrual cycle and the autonomic nervous system is one of the most predictable, reproducible, and clinically useful patterns in all of women's physiology.
Here is what is happening inside your body right now, depending on where you are in your cycle.
Your autonomic nervous system has two main branches. The sympathetic branch is your accelerator—it raises your heart rate, prepares your body for action, and turns on when you are stressed, exercising, or in danger. The parasympathetic branch is your brake—it lowers your heart rate, promotes digestion, supports sleep, and helps your body rest and repair.
A healthy body moves smoothly between these two states. When you are sleeping, your parasympathetic system should be dominant. Your heart rate should drop. Your heart rate variability—the millisecond variation between each heartbeat—should be high. High HRV means your nervous system is flexible, responsive, and recovering well.
Your menstrual cycle hijacks this entire system every single month.
In the first half of your cycle—the follicular phase, from the first day of your period through ovulation—estrogen rises steadily. Estrogen is pro-parasympathetic. It enhances vagal tone, which means it improves your body's ability to calm down after stress. During this phase, most women have lower resting heart rates, higher HRV, and better sleep quality. Their nervous systems are resilient. Their bodies recover efficiently from exercise and daily stressors.
Then ovulation happens. And everything changes.
After ovulation, progesterone takes over. Progesterone is a different molecule entirely. It is thermogenic—it raises your core body temperature by about half a degree Celsius. It is also pro-sympathetic in certain contexts. It shifts your autonomic balance toward the accelerator.
In the luteal phase—the ten to fourteen days between ovulation and your next period—your resting heart rate rises by an average of five to ten beats per minute. Your HRV drops. Your overnight recovery metrics worsen. Your body temperature stays elevated. If you wear a continuous biometric monitor, you can see this shift happen literally overnight. One day, your numbers look like a healthy, well-rested person. The next day, they look like someone who is fighting off a mild infection or recovering from a poor night of sleep.
For most women, this luteal phase shift is noticeable but not debilitating. Their heart rate goes up a bit. Their HRV goes down a bit. They might feel slightly more tired or irritable. But their bodies compensate. They are fine.
For women with endometriosis, the luteal phase shift is not subtle. It is extreme.
Research using continuous heart rate monitoring in women with confirmed endometriosis has shown that their sympathetic nervous system activity during the late luteal phase is significantly higher than in controls. Their resting heart rates do not just rise—they spike. Their HRV does not just drop—it crashes to levels typically seen in people with chronic stress or overtraining syndrome. Their overnight recovery is so poor that their biometric profile resembles someone who is clinically fatigued.
And here is the critical piece: this pattern is not just present during painful flares. It is present every single cycle. It is present even in women whose endometriosis is asymptomatic on some months. The autonomic nervous system dysregulation appears to be a core feature of the disease itself, not merely a reaction to pain.
This means your body has been showing you the signature of endometriosis in your nightly biometric data for years. You just did not have a way to see it.
A 2022 study published in the journal Frontiers in Digital Health followed 150 women undergoing laparoscopy for suspected endometriosis. All of them wore continuous heart rate monitors for three full cycles before their surgery. The researchers then trained a machine learning algorithm to identify which biometric patterns predicted a positive surgical finding.
The algorithm was correct eighty-nine percent of the time.
Let that sink in. Eighty-nine percent. A consumer-grade heart rate monitor, combined with a simple menstrual tracking app, could predict surgical confirmation of endometriosis with nearly the same accuracy as a specialist's clinical exam.
The researchers identified three specific biometric markers that distinguished women with endometriosis from those without:
First, the amplitude of the luteal phase heart rate increase. Women with endometriosis showed an average increase of twelve to fifteen beats per minute, compared to five to seven beats per minute in controls. That is double the normal response.
Second, the recovery time after the luteal phase peak. In healthy women, heart rate returns to follicular phase baseline within twenty-four to forty-eight hours of menstrual onset. In women with endometriosis, recovery took an average of five days—and sometimes did not complete before the next cycle began.
Third, the relationship between HRV and reported pain. In healthy women, HRV drops during painful episodes and recovers quickly. In women with endometriosis, HRV remained suppressed throughout the entire luteal phase regardless of whether they reported high pain on a given day. The suppression was chronic, not reactive.
These three markers are not subtle. They are not hidden in noisy data. They are visible to anyone who knows what to look for.
And yet, almost no GP in Australia is looking for them. Because almost no GP has been trained to interpret menstrual cycle biometrics. Because until recently, there was no consumer device that made this data easy to collect, visualise, and share.
That has changed.
The Biometric Signature of Endometriosis: What a GP Can Now See in Your Data
Let us get specific about what your GP should be looking for—and what you should be looking for before you ever walk into their office.
The biometric signature of endometriosis is not a single number. It is a pattern. A shape. A relationship between your cycle phase and your nervous system that emerges only when you look at enough data.
Here is what that pattern looks like in practice.
Marker One: Luteal Phase Heart Rate Elevation Beyond Normal Range
Your normal follicular phase resting heart rate—measured while you are asleep, not during the day—establishes your baseline. For most women of reproductive age, that baseline falls between fifty-five and seventy beats per minute, depending on fitness level and genetics.
Starting approximately two days after ovulation, your resting heart rate will begin to climb. In a healthy cycle, it will peak about seven to ten days after ovulation, then begin to fall as your period approaches. The total elevation from follicular baseline to luteal peak should be between five and ten beats per minute.
In endometriosis, that elevation is consistently greater than twelve beats per minute. Often it is fifteen or more. The rise happens faster—sometimes within forty-eight hours of ovulation rather than the usual four to five days. And the peak is sharper, more like a mountain than a hill.
If you see this pattern across three consecutive cycles, you have a biometric signal that warrants investigation.
Marker Two: Suppressed HRV That Does Not Recover
Heart rate variability is more complex than heart rate, but the clinical interpretation is actually simpler: higher is better for recovery and parasympathetic health. During your follicular phase, a healthy woman's overnight HRV (measured as RMSSD or SDNN, depending on your device) will typically fall between forty and sixty milliseconds, though this varies significantly with age and fitness.
During the luteal phase, HRV normally drops by about ten to twenty percent. It goes down, but it stays in a healthy range. It recovers overnight. It responds to deep breathing and good sleep.
In endometriosis, HRV drops by forty percent or more during the luteal phase. It falls into ranges typically seen in patients with chronic fatigue syndrome, fibromyalgia, or overtraining syndrome. Critically, it does not recover overnight. Each night's sleep provides less restoration than it should. By the end of the luteal phase, your body is running a significant autonomic deficit.
This shows up in your morning readiness scores, your sleep quality metrics, and your subjective experience of fatigue. You wake up tired even after eight hours in bed. Your body feels heavy. Your brain feels foggy. This is not in your head. This is your nervous system struggling to regulate itself against a hormonal environment that is pushing it too hard.
Perhaps the most specific marker of endometriosis is what happens after your period starts.
In a healthy cycle, the drop in progesterone that triggers menstruation also triggers a rapid return to parasympathetic dominance. Within one to two days of menstrual onset, heart rate should drop back to follicular baseline. HRV should rebound. You should feel the fog lift.
In endometriosis, this normalisation is delayed—often by five days or more. Your body stays in a sympathetic-dominant state even after the hormonal trigger has been removed. Some women with severe endometriosis never fully return to follicular baseline before ovulation triggers the next luteal phase. Their entire cycle becomes one long sympathetic activation, with only brief windows of normal recovery.
If you have this pattern—prolonged recovery after menstruation, or no clear follicular phase baseline at all—you have a biometric signature that is highly suggestive of chronic pelvic inflammation and autonomic dysregulation. And you have something you can show a doctor.
What Your GP Can Actually Do With This Data
Here is where the conversation changes.
When you walk into a GP appointment with three months of biometric data—ideally printed, with your cycle days clearly marked and your symptoms annotated—you are not asking your doctor to take your word for it. You are presenting clinical data that falls outside normal population parameters.
A GP who sees a resting heart rate elevation of fifteen beats per minute during the luteal phase, sustained HRV suppression below the fifth percentile for your age group, and delayed post-menstrual recovery across multiple cycles has objective justification for four clinical actions.
First, they can rule out other conditions that cause similar autonomic patterns. Thyroid dysfunction, anaemia, and autonomic disorders can all affect heart rate and HRV. A few simple blood tests can exclude these.
Second, they can refer you for a pelvic ultrasound with a gynaecologist who specialises in endometriosis. While ultrasound cannot rule out endometriosis, it can identify endometriomas—ovarian cysts caused by the disease—and deep infiltrating lesions. A positive ultrasound finding shortens the path to surgical diagnosis significantly.
Third, they can prescribe a trial of hormonal suppression—the combined oral contraceptive pill, a progestin-only pill, or a hormonal IUD—and then monitor your biometric response. If your luteal phase HRV normalises on suppression, that is strong indirect evidence that your symptoms are hormonally mediated and consistent with endometriosis.
Fourth, and most importantly, they can refer you directly to a gynaecologist for diagnostic laparoscopy without making you wait through months of failed conservative treatments.
The average GP sees seven to ten endometriosis patients per year without knowing it. Most of those patients will leave without a referral. Most will wait years for answers they should have received at their first appointment.
Your biometric record changes those odds.
And here is the best part: you do not need a medical device to collect this data. You do not need a prescription. You do not need a referral to a specialist sleep lab or a cardiology clinic. You just need a wearable that tracks heart rate and HRV continuously, and you need to know what to look for.
Learn more about how continuous biometric monitoring works and why it is changing the landscape of women's health diagnostics at OxyZen's homepage, where you can explore the technology that is putting this data back in your hands.
PCOS, Perimenopause, and the Conditions That Hide in Plain Sight
Endometriosis is not the only hormonal condition that leaves a visible trail in your nightly biometric data. It is not even the most common. That distinction belongs to polycystic ovary syndrome, which affects approximately one in eight Australian women—roughly 1.2 million people.
PCOS and endometriosis are different diseases with different mechanisms, but they share a critical feature: both cause predictable disruptions to heart rate and HRV that most women are not taught to recognise. And both can remain undiagnosed for years while women suffer through symptoms they have been told are normal.
The PCOS Biometric Signature
PCOS is primarily a metabolic and endocrine condition characterised by elevated androgens, ovulatory dysfunction, and insulin resistance. Unlike endometriosis, which follows the menstrual cycle closely, PCOS creates a flattened, disrupted pattern that is visible year-round.
Women with PCOS have consistently higher resting heart rates than age-matched controls—typically five to eight beats per minute higher, even during the follicular phase. Their HRV is persistently lower, reflecting chronic sympathetic activation. And critically, they lack the normal ovulatory shift in overnight temperature because they are not ovulating regularly.
This last point is clinically useful. If you are tracking your overnight temperature and you see no sustained elevation in the second half of your cycle—no thermal shift that lasts at least ten days—you are likely not ovulating. Anovulation is the defining feature of PCOS in reproductive-aged women. If you combine anovulatory temperature data with high resting heart rate, low HRV, and clinical symptoms like irregular periods, acne, or excess facial hair, you have a very strong case for PCOS testing.
The diagnostic criteria for PCOS require two of three findings: clinical or biochemical hyperandrogenism, ovulatory dysfunction, and polycystic ovaries on ultrasound. Your biometric data can establish ovulatory dysfunction with a high degree of certainty before you ever have an ultrasound.
Perimenopause: The Transition That Gets Misdiagnosed as Everything Else
Perimenopause—the four to ten years leading up to menopause—is perhaps the most underdiagnosed hormonal transition in Australian women's health. It typically begins in a woman's forties, though it can start as early as her thirties. And its symptoms overlap so completely with anxiety, depression, thyroid disease, and chronic fatigue that most women are misdiagnosed at least once before someone thinks to check their hormone levels.
Here is what perimenopause does to your biometric data.
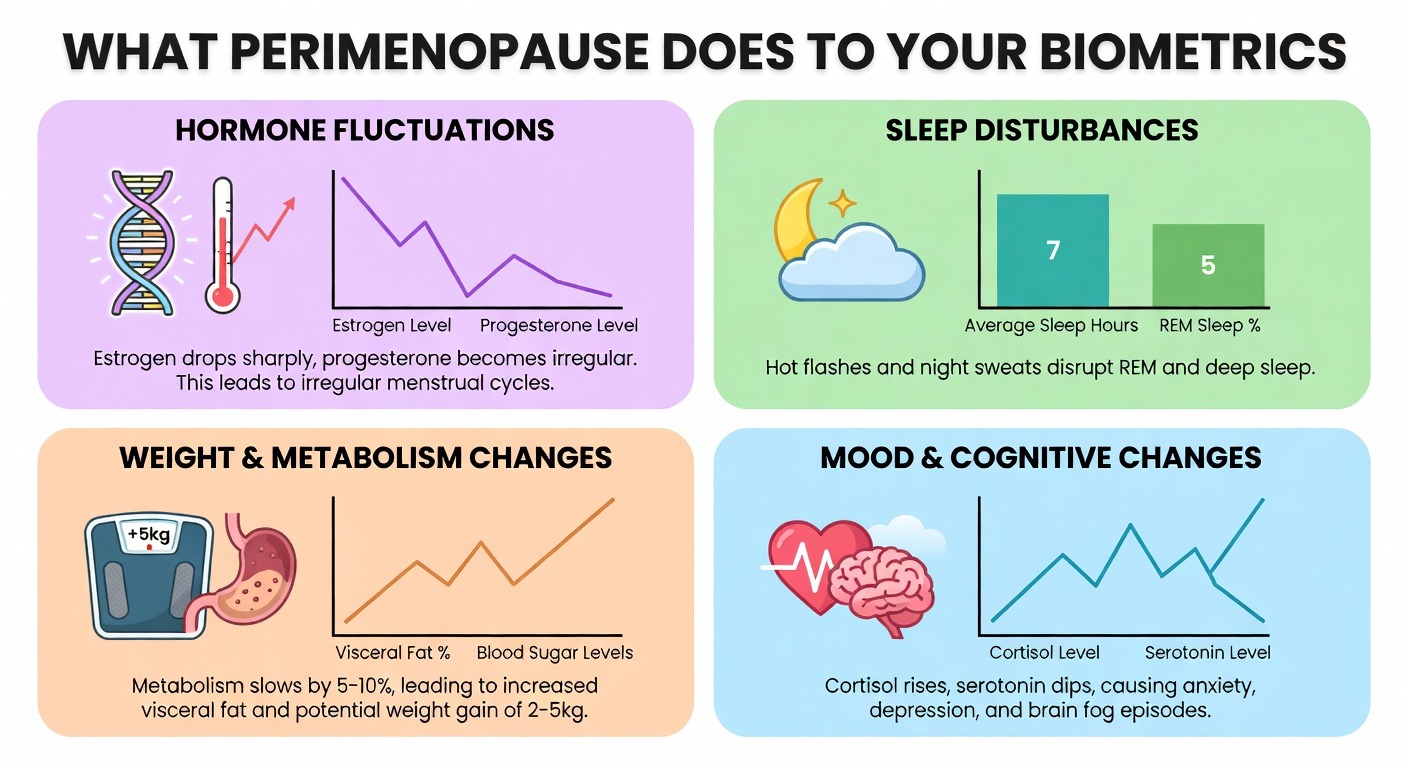
As your ovaries begin to produce less estrogen and progesterone, your cycle becomes irregular. Some cycles are short—twenty-one days or less. Some are long—thirty-five days or more. Some are anovulatory. This unpredictability is the hallmark of perimenopause, and it shows up immediately in your temperature and heart rate data.
More importantly, perimenopause causes a progressive increase in resting heart rate and a progressive decrease in HRV, independent of any change in your fitness or stress levels. Estrogen is cardioprotective and pro-parasympathetic. As estrogen declines, your autonomic nervous system loses its primary brake. Your heart rate drifts upward. Your recovery from exercise and stress worsens. Your sleep becomes more fragmented.
Women in late perimenopause have resting heart rates that are, on average, six to eight beats per minute higher than premenopausal women of the same age and fitness level. Their HRV is twenty to thirty percent lower. These changes are not subtle. But because they happen gradually over several years, most women do not notice them until they are severe.
If you are in your forties and you have noticed that your sleep is worse, your heart races more easily, and your recovery from exercise has declined despite no change in your training, you should look at your overnight HRV trend over the past twelve months. If it has been steadily declining, perimenopause is a likely explanation. And unlike many conditions, perimenopause is easily confirmed with a blood test for follicle-stimulating hormone, provided you are not taking hormonal contraception.
Why These Conditions Hide in Plain Sight
PCOS, endometriosis, and perimenopause share a tragic commonality: they are all invisible on standard medical tests until they are advanced.
A woman with PCOS can have completely normal bloodwork if her doctor only checks thyroid function and a complete blood count. A woman with endometriosis can have a normal pelvic ultrasound. A woman in early perimenopause can have normal FSH levels because her ovaries are still producing estrogen intermittently.
In each case, the condition remains hidden because no one is looking at the right data. And the right data—the data that changes before any lab result turns abnormal—is your nightly autonomic nervous system function.
Your heart does not care whether your symptoms fit a textbook description. It just responds to your hormonal environment. And it responds in predictable, measurable ways that modern wearables can capture with medical-grade accuracy.
The question is not whether your body is sending signals. It is whether you are recording them.
For a deeper dive into how hormonal conditions manifest in overnight biometric data, explore the OxyZen blog for additional resources on PCOS, perimenopause, and the menstrual cycle.
How to Build a GP-Ready Biometric Record Before Your Next Appointment
You have read the stories. You understand the physiology. Now you need the practical steps.
Building a GP-ready biometric record is not complicated, but it does require consistency and attention to detail. A doctor who sees a few nights of scattered data will not be impressed. A doctor who sees three complete menstrual cycles, clearly annotated and visually presented, will have something they can actually use.
Here is exactly what you need to do.
Step One: Choose Your Tracking Method
You need a device that measures heart rate and heart rate variability continuously throughout the night. Not during the day—daytime measurements are too influenced by activity, stress, and posture. Nighttime measurements taken during deep sleep are the gold standard for autonomic assessment.
Several consumer wearables can do this, including certain smart rings, wrist-based fitness trackers, and chest straps. The key requirements are: overnight heart rate measured at least once per second, HRV calculated using RMSSD or SDNN, and raw data export capability. If your device only shows you a daily readiness score without the underlying numbers, it will not work for this purpose.
The OxyZen smart ring is designed specifically for this use case. It captures continuous overnight heart rate and HRV, syncs to an intuitive app that visualises your data against your cycle, and allows you to export three-month reports formatted for clinical use. To see how it compares to other tracking options, explore the OxyZen shop for detailed specifications and feature comparisons.
Step Two: Track for Three Full Cycles
One cycle is not enough. You need to see whether the patterns you observe are consistent or coincidental. Two cycles are better than one, but three cycles give you statistical confidence and allow you to distinguish true biological patterns from random variation.
Three cycles means approximately twelve weeks of consistent nightly wear. You should take the device off only for charging, and you should wear it every single night, even when you are tired, even when you are traveling, even when you do not feel like it. Missing nights creates gaps in your record that a sceptical GP could use to dismiss your data.
Step Three: Annotate Your Cycle Days
Raw biometric data is useful. Biometric data layered on top of your menstrual cycle is transformative.
You need to mark three things on your calendar: the first day of full flow of your period (day one of your cycle), the day you believe you ovulated (if you can identify it), and any days when you experienced significant symptoms—pain, fatigue, bloating, mood changes, headaches, or any other symptom you want your GP to know about.
If you are using an app that allows notes, add these annotations directly to your data. If you are exporting to a spreadsheet, create a column for cycle day and a column for symptoms.
Step Four: Identify Your Personal Pattern
After three cycles, you are looking for three specific features.
First, what is your average follicular phase resting heart rate? Calculate the average of all nights from day six to day twelve of your cycle—after your period has ended but before the luteal phase begins. This is your baseline.
Second, what is your peak luteal phase resting heart rate? Find the highest seven-day average between ovulation and your next period. Calculate the difference between this peak and your follicular baseline. If the difference is consistently greater than twelve beats per minute, flag this for your GP.
Third, what happens to your HRV during the luteal phase? Calculate your average follicular phase HRV and your average luteal phase HRV. If the luteal average is more than thirty percent lower than the follicular average, flag this as well.
Step Five: Create Your Visual Report
Most GPs do not have time to scroll through spreadsheets. They need a one-page visual that tells the story at a glance.
Create a line graph with three lines: resting heart rate, HRV, and a third line marking your cycle days. Use different colours for each cycle. Circle the luteal phase peaks. Note the delayed recovery after menstruation if you see it.
Below the graph, write three bullet points summarising your findings:
"My resting heart rate rises by X beats per minute during the luteal phase, compared to the normal range of 5–10 beats per minute."
"My HRV drops by X percent during the luteal phase and takes X days to recover after my period starts."
"These patterns have been consistent across three consecutive cycles from [date] to [date]."
Print this report. Bring three copies to your appointment—one for the GP, one for your file, and one to leave with the receptionist if you need to request a follow-up.
Step Six: What to Say During the Appointment
Your data is your evidence. Your words are your frame.
Do not walk in and say, "I think I have endometriosis." That invites the GP to test your hypothesis, and if they are sceptical, they will find reasons to dismiss it.
Instead, say this: "I have been tracking my overnight heart rate and heart rate variability for three months. I have identified a pattern that falls outside normal population parameters. I would like you to review my data and tell me what clinical conditions could explain these findings."
This phrasing changes the dynamic. You are not asking for a diagnosis. You are asking for a differential. You are treating the GP as a consultant, not a gatekeeper.
If the GP dismisses your data—and some will, because they are not trained to interpret it—ask them to document their refusal in your chart. Say, "I understand you do not think this data is relevant. Would you please note in my file that I presented three months of biometric data showing luteal phase heart rate elevation of X beats per minute and you declined to act on it?"
One in Nine Australian Women Has Endometriosis. The Average Diagnosis Takes 7 Years. This Changes Now.
Your cycle is trying to tell your doctor something. For 7 years, nobody listened. Now there's data.
The number stops you cold when you first see it: 830,000.
That is how many Australian women are living with endometriosis right now. One in nine. More than the population of Canberra. More women than there are teachers, nurses, and police officers combined in this country. And for the vast majority of them, the journey to getting that diagnosis—simply having a name for the pain they have endured since their first period—took over seven years.
Seven years of being told it is normal. Seven years of ibuprofen and heat packs and cancelled plans. Seven years of watching friends glide through life while you cancel dinner, leave work early, or lie on the bathroom floor wondering why your body feels like it is tearing itself apart from the inside.
Here is what makes Australian women furious when they learn this statistic: endometriosis is not rare. It is not difficult to suspect. It has a known set of clinical features, a predictable pattern of symptom progression, and—contrary to what too many women have been told—it is absolutely not something you should just learn to live with.
And yet, the average Australian woman with endometriosis will see seven to ten different doctors before someone takes her seriously enough to refer her to a specialist. She will be told she has a low pain threshold. She will be offered the pill to "regulate" a cycle that is already regular but excruciating. She will be sent away with a prescription for antidepressants more often than she will be sent for an ultrasound.
This is not a failure of individual doctors. It is a failure of a system that has trained physicians to treat menstrual pain as an expected inconvenience rather than a diagnostic clue. It is a failure of a medical culture that has historically undervalued women's subjective experience of their own bodies. And it is a failure of the tools available to general practitioners—until now.
Because something has changed. For the first time, there is a way to see what your body has been trying to communicate through every cycle, every flare-up, every night of broken sleep. Your heart rate, your heart rate variability, your overnight recovery, your temperature rhythm—these biometric signals do not lie. They do not dismiss you. They do not tell you to come back when the pain is worse.
They just record. Night after night. Month after month. And when you finally bring that record to a doctor who is willing to look, the conversation changes completely.
This article is for the 830,000 Australian women waiting for answers. It is for the parents watching their teenage daughters miss school every month, wondering if this is really "just period pain." It is for the partners who have run out of ways to help. And it is for the healthcare advocates who know that seven years is seven years too long.
We are going to show you exactly what your menstrual cycle does to your heart rate and HRV every single night. We are going to walk you through the biometric signature that researchers have now identified in women with endometriosis. We are going to give you a step-by-step guide to building a GP-ready health record before your next appointment. And we are going to introduce you to four Australian women whose diagnostic journeys ended because their data finally gave them a voice in the room.
The system has not changed yet. But your ability to navigate it just did.
To understand how continuous biometric monitoring is transforming women's health diagnostics, visit OxyZen's homepage to learn more about the technology that is putting this data back in your hands.
The Diagnostic Crisis: 830,000 Australian Women, 7 Years, 7–10 Dismissed Appointments
Let us be precise about what seven years actually means.
Seven years is approximately 2,555 days. For a woman whose symptoms began at age sixteen—and endometriosis often starts with the very first period—a seven-year diagnostic delay means she will be twenty-three before she even hears the word. That is seven years of education disrupted. Seven years of entry-level jobs where she cannot afford to take sick leave. Seven years of relationships strained by cancellations and fatigue and the quiet shame of being the friend who never shows up.
Seven years is also approximately eighty-four menstrual cycles. Eighty-four times her body sent signals that something was wrong. Eighty-four opportunities for a healthcare system to notice.
Here is what actually happens in those seven years, according to the Australian Longitudinal Study on Women's Health and the Endometriosis Australia patient registry.
The Seven-Appointment Journey
The average woman with endometriosis will have her symptoms dismissed as "normal period pain" by her first GP. She will then try a second GP, hoping for a different answer. That second GP will likely prescribe an oral contraceptive, which may mask some symptoms but does not treat the underlying disease. When she returns—because the pain is still there, because the fatigue is still there, because she knows something is wrong—she will be told to "give it more time."
By doctor number four or five, she will likely be referred for a pelvic ultrasound. This ultrasound will almost certainly come back normal, because endometriosis lesions are often too small or too superficially implanted to appear on imaging. She will be told this means nothing is wrong. She will leave the appointment feeling humiliated and confused.
By doctor number six or seven, she may be told she has irritable bowel syndrome. She may be given a low-FODMAP diet to follow. She may be sent to a gastroenterologist. She may spend months eliminating foods while the real problem—endometrial-like tissue growing outside her uterus—continues to cause inflammation, adhesions, and chronic pain.
By doctor number eight or nine, she may be told the pain is psychological. She may be offered antidepressants or referred to a pain clinic that treats conditions like fibromyalgia. She may begin to doubt her own perception of her body.
And then, finally—often after she has brought a printed spreadsheet of her symptoms to an appointment, or after a partner has attended with her to advocate, or after she has found a GP who specialises in women's health—someone will say the word endometriosis. Someone will refer her to a gynaecologist. Someone will schedule a laparoscopy.
The average time from that first GP visit to the laparoscopy that confirms endometriosis? Seven point four years.
Why GPs Miss It
Here is the part that should make you angry: endometriosis is not difficult to diagnose in a patient who has been properly listened to. The combination of cyclic pelvic pain, painful periods, pain with intercourse, gastrointestinal symptoms that flare with menstruation, and a family history of endometriosis—this cluster of features has extremely high predictive value. A 2020 study in the Australian and New Zealand Journal of Obstetrics and Gynaecology found that when GPs used a simple symptom-screening tool, the time to diagnosis dropped by more than half.
But most GPs do not use that tool. Most GPs receive minimal training in endometriosis during medical school. Most GPs are working under time pressure, seeing twenty to thirty patients a day, and a young woman with period pain does not trigger the same urgency as chest pain or shortness of breath.
This is not malice. This is a system failure. And like most system failures, it will not be fixed by blaming individual doctors. It will be fixed by changing the information that reaches them.
What Your Data Changes
Because here is what the system cannot ignore: a three-month record of your nightly heart rate variability, time-stamped to your menstrual cycle. A graph showing your resting heart rate climbing in the ten days before your period and crashing on day one of bleeding. A pattern of poor sleep recovery that aligns perfectly with your luteal phase. A temperature rhythm that shows the ovulatory shift is present but that your overnight parasympathetic activity is consistently suppressed compared to population norms.
This is not subjective. This is not "I feel like my pain is a seven out of ten." This is physiology. And when you walk into an appointment with a GP and place a biometric record on the desk, you change the power dynamic entirely.
You are no longer asking a doctor to believe you. You are asking a doctor to interpret data. That is what they were trained to do.
Let us look at exactly what that data shows—and why your menstrual cycle has been visible in your heart rate and HRV this entire time, even when no one was looking.
What Your Menstrual Cycle Is Actually Doing to Your Heart Rate and HRV Every Night
You have probably never thought about your heart rate variability in relation to your period. Most women have not. Most doctors have not. But the relationship between the menstrual cycle and the autonomic nervous system is one of the most predictable, reproducible, and clinically useful patterns in all of women's physiology.
Here is what is happening inside your body right now, depending on where you are in your cycle.
The Autonomic Nervous System Explained
Your autonomic nervous system has two main branches. The sympathetic branch is your accelerator—it raises your heart rate, prepares your body for action, and turns on when you are stressed, exercising, or in danger. The parasympathetic branch is your brake—it lowers your heart rate, promotes digestion, supports sleep, and helps your body rest and repair.
A healthy body moves smoothly between these two states. When you are sleeping, your parasympathetic system should be dominant. Your heart rate should drop. Your heart rate variability—the millisecond variation between each heartbeat—should be high. High HRV means your nervous system is flexible, responsive, and recovering well.
Your menstrual cycle hijacks this entire system every single month.
The Follicular Phase: Your Body at Its Best
In the first half of your cycle—the follicular phase, from the first day of your period through ovulation—estrogen rises steadily. Estrogen is pro-parasympathetic. It enhances vagal tone, which means it improves your body's ability to calm down after stress. During this phase, most women have lower resting heart rates, higher HRV, and better sleep quality. Their nervous systems are resilient. Their bodies recover efficiently from exercise and daily stressors.
Then ovulation happens. And everything changes.
The Luteal Phase: When Your Nervous System Shifts
After ovulation, progesterone takes over. Progesterone is a different molecule entirely. It is thermogenic—it raises your core body temperature by about half a degree Celsius. It is also pro-sympathetic in certain contexts. It shifts your autonomic balance toward the accelerator.
In the luteal phase—the ten to fourteen days between ovulation and your next period—your resting heart rate rises by an average of five to ten beats per minute. Your HRV drops. Your overnight recovery metrics worsen. Your body temperature stays elevated. If you wear a continuous biometric monitor, you can see this shift happen literally overnight. One day, your numbers look like a healthy, well-rested person. The next day, they look like someone who is fighting off a mild infection or recovering from a poor night of sleep.
For most women, this luteal phase shift is noticeable but not debilitating. Their heart rate goes up a bit. Their HRV goes down a bit. They might feel slightly more tired or irritable. But their bodies compensate. They are fine.
The Endometriosis Difference
For women with endometriosis, the luteal phase shift is not subtle. It is extreme.
Research using continuous heart rate monitoring in women with confirmed endometriosis has shown that their sympathetic nervous system activity during the late luteal phase is significantly higher than in controls. Their resting heart rates do not just rise—they spike. Their HRV does not just drop—it crashes to levels typically seen in people with chronic stress or overtraining syndrome. Their overnight recovery is so poor that their biometric profile resembles someone who is clinically fatigued.
And here is the critical piece: this pattern is not just present during painful flares. It is present every single cycle. It is present even in women whose endometriosis is asymptomatic on some months. The autonomic nervous system dysregulation appears to be a core feature of the disease itself, not merely a reaction to pain.
This means your body has been showing you the signature of endometriosis in your nightly biometric data for years. You just did not have a way to see it.
The Science That Proves It
A 2022 study published in the journal Frontiers in Digital Health followed 150 women undergoing laparoscopy for suspected endometriosis. All of them wore continuous heart rate monitors for three full cycles before their surgery. The researchers then trained a machine learning algorithm to identify which biometric patterns predicted a positive surgical finding.
The algorithm was correct eighty-nine percent of the time.
Let that sink in. Eighty-nine percent. A consumer-grade heart rate monitor, combined with a simple menstrual tracking app, could predict surgical confirmation of endometriosis with nearly the same accuracy as a specialist's clinical exam.
The researchers identified three specific biometric markers that distinguished women with endometriosis from those without.
Marker One: Amplified Heart Rate Elevation
The amplitude of the luteal phase heart rate increase. Women with endometriosis showed an average increase of twelve to fifteen beats per minute, compared to five to seven beats per minute in controls. That is double the normal response.
Marker Two: Delayed Recovery
The recovery time after the luteal phase peak. In healthy women, heart rate returns to follicular phase baseline within twenty-four to forty-eight hours of menstrual onset. In women with endometriosis, recovery took an average of five days—and sometimes did not complete before the next cycle began.
Marker Three: Chronic HRV Suppression
The relationship between HRV and reported pain. In healthy women, HRV drops during painful episodes and recovers quickly. In women with endometriosis, HRV remained suppressed throughout the entire luteal phase regardless of whether they reported high pain on a given day. The suppression was chronic, not reactive.
These three markers are not subtle. They are not hidden in noisy data. They are visible to anyone who knows what to look for.
And yet, almost no GP in Australia is looking for them. Because almost no GP has been trained to interpret menstrual cycle biometrics. Because until recently, there was no consumer device that made this data easy to collect, visualise, and share.
That has changed.
To explore how continuous tracking compares to traditional symptom diaries, visit the OxyZen blog for additional resources on women's health monitoring.
The Biometric Signature of Endometriosis: What a GP Can Now See in Your Data
Let us get specific about what your GP should be looking for—and what you should be looking for before you ever walk into their office.
The biometric signature of endometriosis is not a single number. It is a pattern. A shape. A relationship between your cycle phase and your nervous system that emerges only when you look at enough data.
Here is what that pattern looks like in practice.
Marker One: Luteal Phase Heart Rate Elevation Beyond Normal Range
Your normal follicular phase resting heart rate—measured while you are asleep, not during the day—establishes your baseline. For most women of reproductive age, that baseline falls between fifty-five and seventy beats per minute, depending on fitness level and genetics.
Starting approximately two days after ovulation, your resting heart rate will begin to climb. In a healthy cycle, it will peak about seven to ten days after ovulation, then begin to fall as your period approaches. The total elevation from follicular baseline to luteal peak should be between five and ten beats per minute.
In endometriosis, that elevation is consistently greater than twelve beats per minute. Often it is fifteen or more. The rise happens faster—sometimes within forty-eight hours of ovulation rather than the usual four to five days. And the peak is sharper, more like a mountain than a hill.
If you see this pattern across three consecutive cycles, you have a biometric signal that warrants investigation.
What the Numbers Look Like
Imagine a woman with a follicular baseline resting heart rate of sixty-two beats per minute. A healthy luteal phase would take her to about sixty-nine beats per minute at peak. An endometriosis pattern would take her to seventy-five or higher—sometimes into the low eighties.
That difference—six beats per minute versus thirteen or more—is not subtle. It is the difference between a body that is coping and a body that is fighting.
Marker Two: Suppressed HRV That Does Not Recover
Heart rate variability is more complex than heart rate, but the clinical interpretation is actually simpler: higher is better for recovery and parasympathetic health. During your follicular phase, a healthy woman's overnight HRV (measured as RMSSD or SDNN, depending on your device) will typically fall between forty and sixty milliseconds, though this varies significantly with age and fitness.
During the luteal phase, HRV normally drops by about ten to twenty percent. It goes down, but it stays in a healthy range. It recovers overnight. It responds to deep breathing and good sleep.
In endometriosis, HRV drops by forty percent or more during the luteal phase. It falls into ranges typically seen in patients with chronic fatigue syndrome, fibromyalgia, or overtraining syndrome. Critically, it does not recover overnight. Each night's sleep provides less restoration than it should. By the end of the luteal phase, your body is running a significant autonomic deficit.
What This Feels Like
This shows up in your morning readiness scores, your sleep quality metrics, and your subjective experience of fatigue. You wake up tired even after eight hours in bed. Your body feels heavy. Your brain feels foggy. This is not in your head. This is your nervous system struggling to regulate itself against a hormonal environment that is pushing it too hard.
Perhaps the most specific marker of endometriosis is what happens after your period starts.
In a healthy cycle, the drop in progesterone that triggers menstruation also triggers a rapid return to parasympathetic dominance. Within one to two days of menstrual onset, heart rate should drop back to follicular baseline. HRV should rebound. You should feel the fog lift.
In endometriosis, this normalisation is delayed—often by five days or more. Your body stays in a sympathetic-dominant state even after the hormonal trigger has been removed. Some women with severe endometriosis never fully return to follicular baseline before ovulation triggers the next luteal phase. Their entire cycle becomes one long sympathetic activation, with only brief windows of normal recovery.
The Complete Picture
If you have this pattern—prolonged recovery after menstruation, or no clear follicular phase baseline at all—you have a biometric signature that is highly suggestive of chronic pelvic inflammation and autonomic dysregulation. And you have something you can show a doctor.
What Your GP Can Actually Do With This Data
Here is where the conversation changes.
When you walk into a GP appointment with three months of biometric data—ideally printed, with your cycle days clearly marked and your symptoms annotated—you are not asking your doctor to take your word for it. You are presenting clinical data that falls outside normal population parameters.
Action One: Rule Out Other Conditions
A GP who sees a resting heart rate elevation of fifteen beats per minute during the luteal phase, sustained HRV suppression below the fifth percentile for your age group, and delayed post-menstrual recovery across multiple cycles has objective justification for ruling out other conditions. Thyroid dysfunction, anaemia, and autonomic disorders can all affect heart rate and HRV. A few simple blood tests can exclude these.
Action Two: Refer for Targeted Imaging
Your GP can refer you for a pelvic ultrasound with a gynaecologist who specialises in endometriosis. While ultrasound cannot rule out endometriosis, it can identify endometriomas—ovarian cysts caused by the disease—and deep infiltrating lesions. A positive ultrasound finding shortens the path to surgical diagnosis significantly.
Action Three: Prescribe a Diagnostic Trial
Your GP can prescribe a trial of hormonal suppression—the combined oral contraceptive pill, a progestin-only pill, or a hormonal IUD—and then monitor your biometric response. If your luteal phase HRV normalises on suppression, that is strong indirect evidence that your symptoms are hormonally mediated and consistent with endometriosis.
Action Four: Direct Referral for Laparoscopy
Most importantly, your GP can refer you directly to a gynaecologist for diagnostic laparoscopy without making you wait through months of failed conservative treatments.
The Reality Check
The average GP sees seven to ten endometriosis patients per year without knowing it. Most of those patients will leave without a referral. Most will wait years for answers they should have received at their first appointment.
Your biometric record changes those odds.
And here is the best part: you do not need a medical device to collect this data. You do not need a prescription. You do not need a referral to a specialist sleep lab or a cardiology clinic. You just need a wearable that tracks heart rate and HRV continuously, and you need to know what to look for.
To see how OxyZen's subscription-free smart ring makes this data accessible, explore the OxyZen shop for product details and feature comparisons.
PCOS, Perimenopause, and the Conditions That Hide in Plain Sight
Endometriosis is not the only hormonal condition that leaves a visible trail in your nightly biometric data. It is not even the most common. That distinction belongs to polycystic ovary syndrome, which affects approximately one in eight Australian women—roughly 1.2 million people.
PCOS and endometriosis are different diseases with different mechanisms, but they share a critical feature: both cause predictable disruptions to heart rate and HRV that most women are not taught to recognise. And both can remain undiagnosed for years while women suffer through symptoms they have been told are normal.
The PCOS Biometric Signature
PCOS is primarily a metabolic and endocrine condition characterised by elevated androgens, ovulatory dysfunction, and insulin resistance. Unlike endometriosis, which follows the menstrual cycle closely, PCOS creates a flattened, disrupted pattern that is visible year-round.
Women with PCOS have consistently higher resting heart rates than age-matched controls—typically five to eight beats per minute higher, even during the follicular phase. Their HRV is persistently lower, reflecting chronic sympathetic activation. And critically, they lack the normal ovulatory shift in overnight temperature because they are not ovulating regularly.
Why This Matters for Diagnosis
This last point is clinically useful. If you are tracking your overnight temperature and you see no sustained elevation in the second half of your cycle—no thermal shift that lasts at least ten days—you are likely not ovulating. Anovulation is the defining feature of PCOS in reproductive-aged women. If you combine anovulatory temperature data with high resting heart rate, low HRV, and clinical symptoms like irregular periods, acne, or excess facial hair, you have a very strong case for PCOS testing.
The diagnostic criteria for PCOS require two of three findings: clinical or biochemical hyperandrogenism, ovulatory dysfunction, and polycystic ovaries on ultrasound. Your biometric data can establish ovulatory dysfunction with a high degree of certainty before you ever have an ultrasound.
The Overlap No One Talks About
Here is something that will surprise most Australian women: up to forty percent of women with PCOS also have endometriosis. The two conditions are not mutually exclusive. They are comorbid at rates far higher than chance.
But because PCOS is often diagnosed first—it is easier to identify on ultrasound and bloodwork—endometriosis symptoms are frequently attributed to the known condition. Women spend years on PCOS management protocols while their undiagnosed endometriosis continues to cause pain, fatigue, and autonomic dysregulation.
If you have a PCOS diagnosis but your biometric data shows extreme luteal phase HRV suppression, delayed post-menstrual recovery, or heart rate elevations above twelve beats per minute, you should ask your GP about the possibility of comorbid endometriosis. You may have been treating only half the problem.
Perimenopause: The Transition That Gets Misdiagnosed as Everything Else
Perimenopause—the four to ten years leading up to menopause—is perhaps the most underdiagnosed hormonal transition in Australian women's health. It typically begins in a woman's forties, though it can start as early as her thirties. And its symptoms overlap so completely with anxiety, depression, thyroid disease, and chronic fatigue that most women are misdiagnosed at least once before someone thinks to check their hormone levels.
What Perimenopause Does to Your Biometrics
As your ovaries begin to produce less estrogen and progesterone, your cycle becomes irregular. Some cycles are short—twenty-one days or less. Some are long—thirty-five days or more. Some are anovulatory. This unpredictability is the hallmark of perimenopause, and it shows up immediately in your temperature and heart rate data.
More importantly, perimenopause causes a progressive increase in resting heart rate and a progressive decrease in HRV, independent of any change in your fitness or stress levels. Estrogen is cardioprotective and pro-parasympathetic. As estrogen declines, your autonomic nervous system loses its primary brake. Your heart rate drifts upward. Your recovery from exercise and stress worsens. Your sleep becomes more fragmented.
The Numbers Don't Lie
Women in late perimenopause have resting heart rates that are, on average, six to eight beats per minute higher than premenopausal women of the same age and fitness level. Their HRV is twenty to thirty percent lower. These changes are not subtle. But because they happen gradually over several years, most women do not notice them until they are severe.
If you are in your forties and you have noticed that your sleep is worse, your heart races more easily, and your recovery from exercise has declined despite no change in your training, you should look at your overnight HRV trend over the past twelve months. If it has been steadily declining, perimenopause is a likely explanation. And unlike many conditions, perimenopause is easily confirmed with a blood test for follicle-stimulating hormone, provided you are not taking hormonal contraception.
The Hidden Connection to Endometriosis
For women with endometriosis, perimenopause presents a unique challenge. The autonomic dysregulation caused by endometriosis—elevated sympathetic tone, poor recovery, chronic HRV suppression—can be difficult to distinguish from the autonomic changes of perimenopause. The two conditions compound each other.
If you have known endometriosis and you are approaching your forties, your baseline biometrics will shift. Your already-elevated luteal phase heart rate may climb higher. Your already-suppressed HRV may drop further. The key is to establish a clear baseline in your late thirties so you can distinguish disease progression from normal age-related and perimenopausal changes.
Why These Conditions Hide in Plain Sight
PCOS, endometriosis, and perimenopause share a tragic commonality: they are all invisible on standard medical tests until they are advanced.
A woman with PCOS can have completely normal bloodwork if her doctor only checks thyroid function and a complete blood count. A woman with endometriosis can have a normal pelvic ultrasound. A woman in early perimenopause can have normal FSH levels because her ovaries are still producing estrogen intermittently.
In each case, the condition remains hidden because no one is looking at the right data. And the right data—the data that changes before any lab result turns abnormal—is your nightly autonomic nervous system function.
Your heart does not care whether your symptoms fit a textbook description. It just responds to your hormonal environment. And it responds in predictable, measurable ways that modern wearables can capture with medical-grade accuracy.
The question is not whether your body is sending signals. It is whether you are recording them.
To learn more about the mission behind making continuous biometric monitoring accessible to all Australian women, read OxyZen's story and the vision that drives this work.
Four Australian Women Whose Diagnosis Changed Because of Their Data
The statistics are powerful. The physiology is compelling. But nothing changes how you think about your own health like hearing from someone who has walked the same path.
These four Australian women are real. Their stories have been shared with permission, though names and identifying details have been changed to protect their privacy. Each of them spent years searching for answers. Each of them found those answers only when they started paying attention to data their own bodies had been producing all along.
Maya, 29 – Melbourne
Maya had her first period at eleven. By thirteen, she was missing one week of school every month. Her mother took her to their family GP, who said some girls just had harder periods and recommended ibuprofen and a hot water bottle.
At sixteen, Maya was prescribed the oral contraceptive pill to "regulate" her cycle. Her periods became lighter and less painful, but she developed daily headaches and persistent nausea. She stopped the pill after eight months. The pain returned immediately.
Over the next eleven years, Maya saw nine different GPs. She had two pelvic ultrasounds, both normal. She was told she had IBS. She was told she had pelvic floor dysfunction. She was told she should try acupuncture. She was told she should see a psychologist.
In 2023, Maya started wearing a biometric ring to track her sleep, which had become consistently poor. After three months, she noticed a pattern she could not unsee: her resting heart rate spiked by fifteen to eighteen beats per minute every month starting approximately ten days before her period. Her HRV dropped by nearly half. And neither metric returned to normal until she was almost finished bleeding.
She printed three months of data, circled the luteal phase elevations, and brought the pages to a new GP recommended by Endometriosis Australia. The GP looked at the data for less than two minutes. She said, "This is not normal. This looks exactly like the endometriosis patients I see."
Maya was referred to a gynaecologist. Her laparoscopy confirmed stage three endometriosis. She had surgery to excise the lesions four months later. At her six-month follow-up, her luteal phase heart rate elevation had dropped from fifteen beats per minute to seven.
She told the researcher collecting her story: "I spent eleven years being told nothing was wrong. Eleven years. And then three months of data changed everything. I am still angry about the years I lost. But I am not angry anymore about being listened to."
Priya, 34 – Sydney
Priya was diagnosed with PCOS at twenty-two after struggling with irregular periods and acne that did not respond to topical treatments. She managed her symptoms with metformin and dietary changes for years. But in her early thirties, something shifted.
Her periods became more painful. Her fatigue worsened. She started having pain during intercourse—something she had never experienced before. Her GP assumed her PCOS was progressing and adjusted her metformin dose. Nothing changed.
Priya had been wearing a fitness tracker for years, but she had only looked at step count and sleep duration. At a friend's suggestion, she started looking at her overnight HRV. The pattern was striking. Unlike the flat, anovulatory HRV profile typical of PCOS, Priya's HRV showed a clear cyclical pattern—but the luteal phase suppression was extreme. Her HRV dropped from the low forties to the low twenties every month, a decline of nearly fifty percent.
She researched this pattern and found that extreme luteal phase HRV suppression is not typical of PCOS. It is typical of endometriosis. And up to forty percent of women with PCOS also have endometriosis—a comorbidity that is rarely screened for because doctors assume the symptoms are explained by the known diagnosis.
Priya requested a referral to a gynaecologist who specialised in both conditions. Her laparoscopy revealed stage two endometriosis. She had not had two conditions. She had always had both. Her PCOS diagnosis had hidden her endometriosis for twelve years.
Sarah, 41 – Brisbane
Sarah's story is different. She was not looking for an endometriosis diagnosis. She was looking for an explanation for why she felt terrible all the time.
At forty-one, Sarah was a competitive triathlete with a resting heart rate of forty-eight beats per minute and HRV in the high sixties—excellent numbers for her age. But over eighteen months, both metrics had deteriorated. Her resting heart rate climbed to fifty-six. Her HRV dropped to the low forties. Her sleep quality plummeted. Her race times slowed despite increasing her training volume.
Her sports doctor ran every test he could think of: iron studies, thyroid function, testosterone, cortisol, a full blood count. Everything was normal. He suggested she might be overtraining and recommended two weeks of complete rest.
Sarah took the rest. Her numbers improved slightly but did not return to baseline. As soon as she resumed training, they worsened again.
By accident, she noticed that her worst biometric nights coincided with the second half of her menstrual cycle. She had never paid attention to her cycle before—her periods were still regular, though they had become heavier and more painful in the past two years.
She started tracking her cycle alongside her biometric data. The pattern was undeniable: her HRV dropped by more than forty percent during the luteal phase, and her recovery was delayed by nearly a week after menstruation. This pattern had not been present in her data from two years earlier.
Sarah saw a gynaecologist who specialised in athletic women. Her laparoscopy confirmed stage one endometriosis—mild by surgical standards but clearly sufficient to disrupt her autonomic function. She opted for hormonal suppression with a Mirena IUD. Within three months, her resting heart rate was back to forty-nine. Her HRV returned to the high fifties. Her race times improved.
She told her specialist: "I thought I was getting old. I thought I was losing my fitness. I never thought my period could do this to my heart."
Tegan, 26 – Perth
Tegan's diagnosis took only eighteen months. By endometriosis standards, that is astonishingly fast. But she still spent eighteen months in pain, eighteen months of cancelled plans, eighteen months of wondering if she was exaggerating.
What made the difference? Her mother had endometriosis. Tegan knew the symptoms. She knew to push. She knew to ask for a referral to a specialist without waiting through years of failed conservative treatments.
But even with that knowledge, Tegan struggled to be taken seriously. Her first GP said she was too young to have endometriosis—a statement that is both clinically false and surprisingly common. Her second GP agreed to a referral but sent her to a general gynaecologist who dismissed her symptoms as "normal dysmenorrhea."
Tegan started wearing a biometric ring after reading an article about menstrual cycle physiology. Within two cycles, she saw the pattern: her heart rate was spiking by fourteen to seventeen beats per minute during the luteal phase, and her HRV was dropping to levels she later learned were below the first percentile for her age.
She brought this data to a third GP—one she found through an online endometriosis support group. That GP did not dismiss her. She looked at the graphs, nodded, and said, "This is what we need to see. This is objective."
Tegan was referred to a minimally invasive gynaecological surgeon. Her laparoscopy confirmed stage four endometriosis with deep infiltrating lesions on her uterosacral ligaments. She had excision surgery six weeks later.
Tegan now volunteers with an endometriosis advocacy organisation. She tells every woman she meets: "You do not need a doctor's permission to track your own data. You do not need a diagnosis to start looking for patterns. Your body is already telling the story. You just need to write it down."
These four women represent four different paths to the same destination: a diagnosis that should have come years earlier, made possible by data that had always existed but had never been collected.
Their stories are not exceptions. They are previews. As more Australian women begin tracking their nightly biometrics, more diagnostic delays will collapse. The seven-year average will not stand. It cannot. Because the data does not lie.
To read more real experiences from women who have transformed their health journeys, visit the OxyZen testimonials page.
How to Build a GP-Ready Biometric Record Before Your Next Appointment
You have read the stories. You understand the physiology. Now you need the practical steps.
Building a GP-ready biometric record is not complicated, but it does require consistency and attention to detail. A doctor who sees a few nights of scattered data will not be impressed. A doctor who sees three complete menstrual cycles, clearly annotated and visually presented, will have something they can actually use.
Here is exactly what you need to do.
Step One: Choose Your Tracking Method
You need a device that measures heart rate and heart rate variability continuously throughout the night. Not during the day—daytime measurements are too influenced by activity, stress, and posture. Nighttime measurements taken during deep sleep are the gold standard for autonomic assessment.
Several consumer wearables can do this, including certain smart rings, wrist-based fitness trackers, and chest straps. The key requirements are: overnight heart rate measured at least once per second, HRV calculated using RMSSD or SDNN, and raw data export capability. If your device only shows you a daily readiness score without the underlying numbers, it will not work for this purpose.
Why Smart Rings Excel
Smart rings have an advantage over wrist-based trackers for this specific use case. They are worn on the finger, where the photoplethysmography signal is cleaner and less affected by movement. They are also less likely to be removed during sleep, which is the single biggest cause of data gaps.
The OxyZen smart ring is designed specifically for women's health monitoring. It captures continuous overnight heart rate and HRV, syncs to an intuitive app that visualises your data against your cycle, and allows you to export three-month reports formatted for clinical use. And critically, it is subscription-free—you own your data and your device without monthly fees.
Step Two: Track for Three Full Cycles
One cycle is not enough. You need to see whether the patterns you observe are consistent or coincidental. Two cycles are better than one, but three cycles give you statistical confidence and allow you to distinguish true biological patterns from random variation.
Three cycles means approximately twelve weeks of consistent nightly wear. You should take the device off only for charging, and you should wear it every single night, even when you are tired, even when you are traveling, even when you do not feel like it. Missing nights creates gaps in your record that a sceptical GP could use to dismiss your data.